Birajdar Anteshwar, Kumar Sushant, Phalak Mukesh, Chaudhari Tushar, Meghana Damarla
Dr. D. Y. Patil Medical Hospital and Research Centre, Pimpri Chinchwad, Pune, Maharashtra, India.
J Orthop Case Rep. 2025 Jan;15(1):254-259. doi: 10.13107/jocr.2025.v15.i01.5192.
The peripheral radioulnar articulation and the bony radioulnar articulation make up the distal radioulnar joint (DRUJ), a diarthrodial trochoid synovial joint stabilizers for soft tissues. Of the DRUJ's stability, only around 20% may be attributed to the bony articulation. Treatment for DRUJ injuries resulting from a solely ligamentous rupture varies and is subject to debate. Usually, non-operative care is coupled with occupational therapy, activity modification, brace or splint immobilization, and pain management.
The aim of this study was to analyze comprehensive management approaches for acute DRUJ instability post-distal radius fracture.The key takeaway from the article is that TFCC repair may not be essential, with K-wire stabilization providing better range of motion and cast immobilization offering stronger grip, but further large-scale controlled trials are required to fully assess these treatment options in terms of patient satisfaction and functional outcomes.
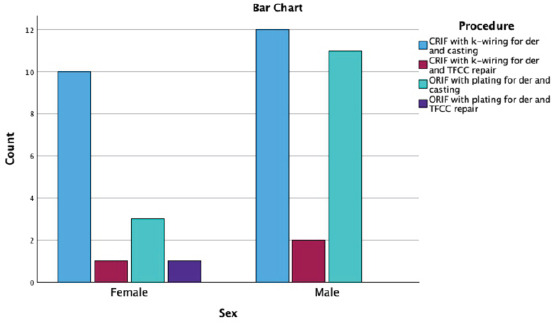
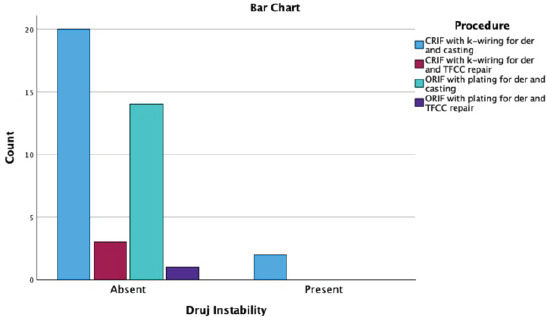
After primary fixation of the respective fractures (distal end radius fracture or distal end ulna fracture or both) by ORIF with Plating or CRIF with K-wiring or by Traction for casting, the distal radio ulna joint instability is stabilized by casting, closed reduction internal fixation (CRIF) with K-wiring or open triangular fibrocartilage complex (TFCC) repair and the outcome is measured by grip strength, range of motion with DASH and MMWS scores by follow up and compared.
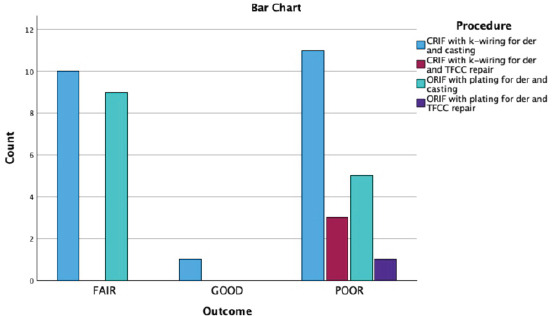
Between the groups, there was no discernible variation in grip strength (P > 0.05). A noteworthy variation in flexion was seen among the groups (P < 0.05). The groups' differences in extension were statistically significant (P < 0.05). Pronation did not significantly differ across the groups (P > 0.05). Supination did not differ significantly between the groups (P > 0.05). The DASH scores of the groups did not differ significantly (P > 0.05). Between the groups, there was a significant difference in MMWS (P < 0.05).
The major findings of analysis have suggested that the time, effort, and cost of TFCC repair do not appear to be necessary, however, there may be trade-offs between various treatments, with K-wire stabilization offering a better range of motion and cast immobilization a stronger grip.
外周桡尺关节和骨性桡尺关节共同构成了下尺桡关节(DRUJ),它是一种滑膜关节,由软组织稳定。在下尺桡关节的稳定性中,只有约20%可归因于骨性关节。对于单纯韧带断裂导致的下尺桡关节损伤,治疗方法各异且存在争议。通常,非手术治疗结合职业治疗、调整活动、使用支具或夹板固定以及疼痛管理。
本研究的目的是分析桡骨远端骨折后急性下尺桡关节不稳定的综合管理方法。本文的关键要点是,三角纤维软骨复合体(TFCC)修复可能并非必要,克氏针固定可提供更好的活动范围,而石膏固定可提供更强的握力,但需要进一步的大规模对照试验,以根据患者满意度和功能结果全面评估这些治疗选择。
通过钢板切开复位内固定(ORIF)、克氏针闭合复位内固定(CRIF)或牵引石膏固定对各自骨折(桡骨远端骨折或尺骨远端骨折或两者皆有)进行初步固定后,通过石膏固定、克氏针闭合复位内固定(CRIF)或开放三角纤维软骨复合体(TFCC)修复来稳定下尺桡关节不稳定,并通过握力、使用DASH和MMWS评分评估随访时的活动范围来测量结果并进行比较。
各组之间握力无明显差异(P>0.05)。各组之间在屈曲方面存在显著差异(P<0.05)。各组在伸展方面的差异具有统计学意义(P<0.05)。各组之间旋前无显著差异(P>0.05)。各组之间旋后无显著差异(P>0.05)。各组的DASH评分无显著差异(P>0.05)。各组之间MMWS存在显著差异(P<0.05)。
分析的主要结果表明,TFCC修复所需的时间、精力和成本似乎并非必要,然而,各种治疗方法之间可能存在权衡,克氏针固定可提供更好的活动范围,而石膏固定握力更强。