Malherbe Stephanus T, Chen Ray Y, Yu Xiang, Smith Bronwyn, Liu Xin, Gao Jingcai, Diacon Andreas H, Dawson Rodney, Tameris Michele, Zhu Hong, Qu Yahong, Jin Hongjian, Pan Shouguo, Dodd Lori E, Wang Jing, Goldfeder Lisa C, Cai Ying, Arora Kriti, Vincent Joel, Narunsky Kim, Serole Keboile, Goliath Rene T, Da Costa Laylah, Taliep Arshad, Aziz Saalikha, Daroowala Remy, Thienemann Friedrich, Mukasa Sandra, Court Richard, Sossen Bianca, Ahlers Petri, Mendelsohn Simon C, White Lisa, Gouel Aurélie, Lau Chuen-Yen, Hassan Samy, Liang Lili, Duan Hongfei, Moghaddam Gita K, Paripati Praveen, Lahouar Saher, Harris Michael, Wollenberg Kurt, Jeffrey Brendan, Tartakovsky Mike, Rosenthal Alex, Duvenhage Michael, Armstrong Derek T, Song Taeksun, Winter Jill, Gao Qian, Via Laura E, Wilkinson Robert J, Walzl Gerhard, Barry Clifton E
DST-NRF Centre of Excellence for Biomedical Tuberculosis Research, South African Medical Research Council Centre for Tuberculosis Research, Division of Immunology, Department of Biomedical Sciences, Faculty of Medicine and Health Sciences, Stellenbosch University, Cape Town, South Africa.
Tuberculosis Research Section, Laboratory of Clinical Immunology and Microbiology, Division of Intramural Research, National Institute of Allergy and Infectious Disease, National Institutes of Health, Bethesda, MD, USA.
medRxiv. 2024 Oct 4:2024.10.03.24314723. doi: 10.1101/2024.10.03.24314723.
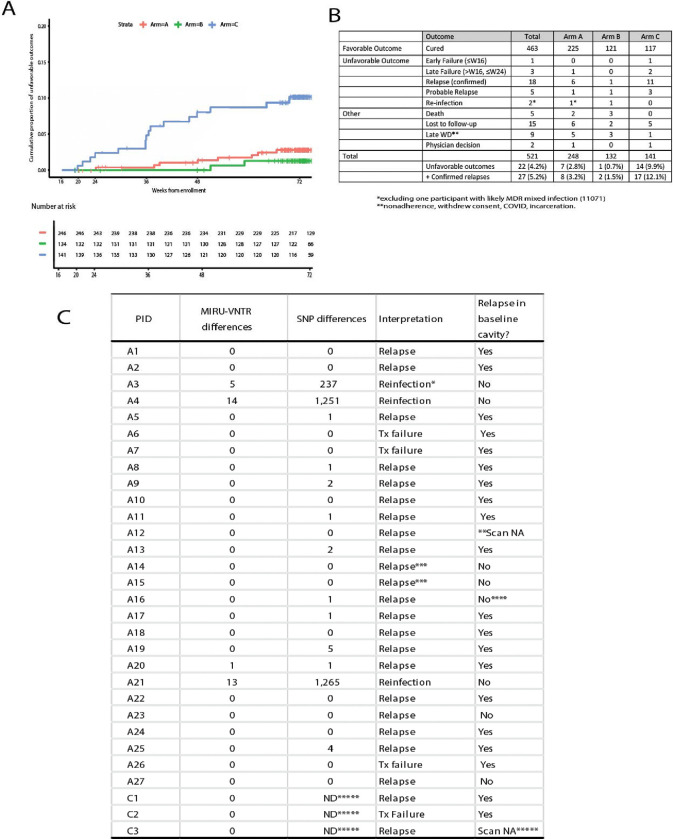
Six months of chemotherapy using current agents is standard of care for pulmonary, drug-sensitive tuberculosis (TB), even though some are believed to be cured more rapidly and others require longer therapy. Understanding what factors determine the length of treatment required for durable cure in individual patients would allow individualization of treatment durations, provide better clinical tools to determine the of appropriate duration of new regimens, as well as reduce the cost of large Phase III studies to determine the optimal combinations to use in TB control programs. We conducted a randomized clinical trial in South Africa and China that recruited 704 participants with newly diagnosed, drug-sensitive pulmonary tuberculosis and stratified them based on radiographic disease characteristics as assessed by FDG PET/CT scan readers. Participants with less extensive disease (N=273) were randomly assigned to complete therapy after four months or continue receiving treatment for six months. Amongst participants who received four months of therapy, 17 of 141 (12.1%) experienced unfavorable outcomes compared to only 2 of 132 (1.5%) who completed six months of treatment (treatment success 98.4% in B, 86.7% in C (difference -11.7%, 95% CI, -18.2%, -5.3%)). In the non-randomized arm that included participants with more extensive disease, only 8 of 248 (3.2%) experienced unfavorable outcomes. Total cavity volume and total lesion glycolysis at week 16 were significantly associated with risk of unfavorable outcome in the randomized participants. Based on PET/CT scans at TB recurrence, bacteriological relapses (confirmed by whole genome sequencing) predominantly occurred in the same active cavities originally present at baseline. Automated segmentation of the serial PET/CT scans was later performed, and machine-learning was used to classify participants according to their likelihood of relapse, allowing the development of predictive models with good performance based on CT, PET, microbiological and clinical characteristics. These results open the possibility for more efficient studies of future TB treatment regimens.
使用现有药物进行六个月的化疗是肺部药敏性结核病(TB)的标准治疗方案,尽管有些人认为可以更快治愈,而另一些人则需要更长时间的治疗。了解哪些因素决定个体患者实现持久治愈所需的治疗时长,将有助于实现治疗时长的个体化,提供更好的临床工具来确定新治疗方案的合适时长,并降低大型III期研究的成本,以确定结核病控制项目中使用的最佳组合。我们在南非和中国进行了一项随机临床试验,招募了704名新诊断的药敏性肺结核患者,并根据FDG PET/CT扫描读取器评估的影像学疾病特征对他们进行分层。疾病范围较小的参与者(N = 273)被随机分配在四个月后完成治疗或继续接受六个月的治疗。在接受四个月治疗的参与者中,141人中有17人(12.1%)出现不良结局,而完成六个月治疗的132人中只有2人(1.5%)出现不良结局(B组治疗成功率为98.4%,C组为86.7%(差异为-11.7%,95% CI,-18.2%,-5.3%))。在包括疾病范围更广的参与者的非随机组中,248人中有8人(3.2%)出现不良结局。第16周时的总空洞体积和总病变糖酵解与随机分组参与者出现不良结局的风险显著相关。基于结核病复发时的PET/CT扫描,细菌学复发(通过全基因组测序确认)主要发生在基线时最初存在的相同活动性空洞中。随后对系列PET/CT扫描进行了自动分割,并使用机器学习根据参与者的复发可能性对其进行分类,从而能够基于CT、PET、微生物学和临床特征开发出性能良好的预测模型。这些结果为未来结核病治疗方案的更高效研究开辟了可能性。