Yun Won-Gun, Chae Yoon Soo, Han Youngmin, Jung Hye-Sol, Cho Young Jae, Kang Hyun-Cheol, Kwon Wooil, Park Joon Seong, Chie Eui Kyu, Jang Jin-Young
Department of Surgery, Seoul National University College of Medicine, 101 Daehak-ro, Jongno-gu, Seoul, 03080, Republic of Korea.
Cancer Research Institute, Seoul National University College of Medicine, Seoul, Republic of Korea.
Ann Surg Oncol. 2025 Apr;32(4):2819-2829. doi: 10.1245/s10434-024-16743-2. Epub 2025 Jan 14.
Benefits of neoadjuvant treatment for pancreatic cancer with major vessel invasion has been demonstrated through randomized controlled trials; however, the optimal neoadjuvant treatment strategy remains controversial, especially for radiotherapy. Therefore, we aimed to evaluate the efficacy and safety of neoadjuvant radiotherapy followed by chemotherapy and the optimal time interval to undergo surgery after radiotherapy in (borderline) resectable pancreatic cancer.
Between 2013 and 2022, patients with (borderline) resectable pancreatic cancer with vessel contact who received 5-fluorouracil with leucovorin, oxaliplatin, and irinotecan or gemcitabine and nanoparticle albumin-bound paclitaxel as initial treatment following surgery were included. Patients who received radiotherapy after chemotherapy and those who did not were matched using 1:1 nearest-neighbor propensity scores. Propensity scores were measured using the tumor size at initial image, duration of neoadjuvant chemotherapy, and responsiveness to neoadjuvant chemotherapy.
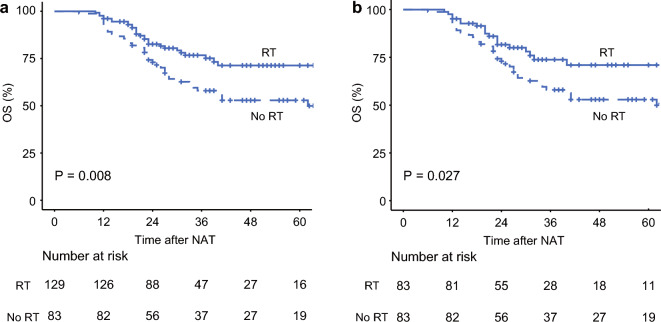
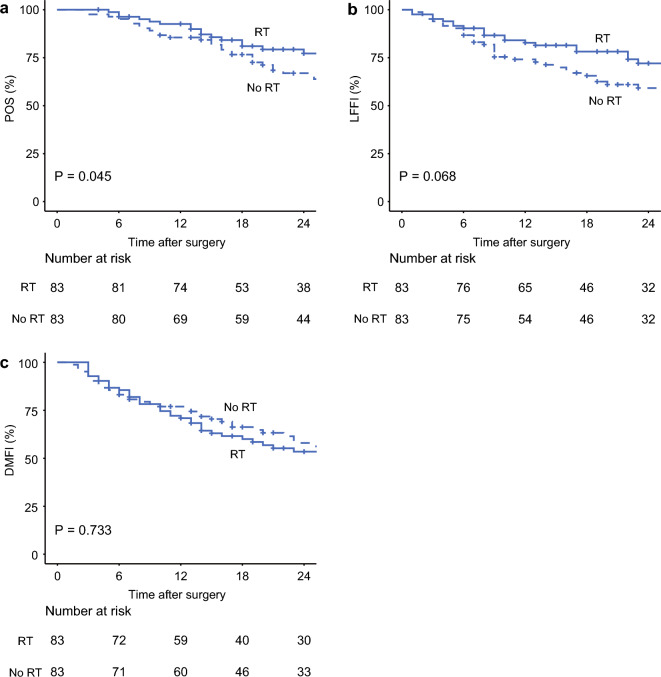
Of 212 patients, 166 patients were retrieved for the matched cohort. Patients who received radiotherapy had significantly better postoperative survival, local control, and R0 resection rates than those who did not. Furthermore, patients who underwent surgery within 4 weeks after completing radiotherapy had lower intraoperative blood loss and a clinically relevant postoperative pancreatic fistula rate than those who underwent surgery after more than 4 weeks.
In patients with (borderline) resectable pancreatic cancer with vessel contact who were scheduled for curative-intent surgery after neoadjuvant chemotherapy, additional radiotherapy was associated with better postoperative survival and local control. Furthermore, our findings suggested that scheduling surgery within 4 weeks following radiation therapy might enhance the perioperative outcomes.
随机对照试验已证实新辅助治疗对伴有大血管侵犯的胰腺癌有益;然而,最佳的新辅助治疗策略仍存在争议,尤其是放射治疗。因此,我们旨在评估新辅助放疗后化疗的疗效和安全性,以及(临界可切除)胰腺癌放疗后进行手术的最佳时间间隔。
纳入2013年至2022年间伴有血管受累的(临界可切除)胰腺癌患者,这些患者在手术后接受了5-氟尿嘧啶联合亚叶酸钙、奥沙利铂和伊立替康,或吉西他滨和纳米白蛋白结合型紫杉醇作为初始治疗。使用1:1最近邻倾向评分对化疗后接受放疗和未接受放疗的患者进行匹配。倾向评分通过初始影像时的肿瘤大小、新辅助化疗持续时间和对新辅助化疗的反应性来衡量。
212例患者中,166例患者被纳入匹配队列。接受放疗的患者术后生存率、局部控制率和R0切除率均显著高于未接受放疗的患者。此外,放疗结束后4周内接受手术的患者术中出血量低于放疗结束4周后接受手术的患者,且术后临床相关胰瘘发生率更低。
对于新辅助化疗后计划进行根治性手术的伴有血管受累的(临界可切除)胰腺癌患者,额外的放疗与更好的术后生存率和局部控制相关。此外,我们的研究结果表明,放疗后4周内安排手术可能会改善围手术期结局。