Weidhase Lorenz, Borrmann Antonia, Willenberg Anja, Mende Meinhard, Scharf-Janßen Christina, Petros Sirak, de Fallois Jonathan
Medical Intensive Care Unit, University Hospital Leipzig, Leipzig, Germany.
Institute for Laboratory Medicine, Clinical Chemistry and Molecular Diagnostics, University Hospital Leipzig, Leipzig, Germany.
BMC Nephrol. 2025 Jan 14;26(1):23. doi: 10.1186/s12882-025-03945-3.
Rhabdomyolysis is frequently associated with acute kidney injury (AKI). Due to the nephrotoxic properties of myoglobin, its rapid removal is relevant. If kidney replacement therapy (KRT) is necessary for AKI, a procedure with effective myoglobin elimination should be preferred. This pilot trial was designed to compare different KRT modes that enable myoglobin elimination.
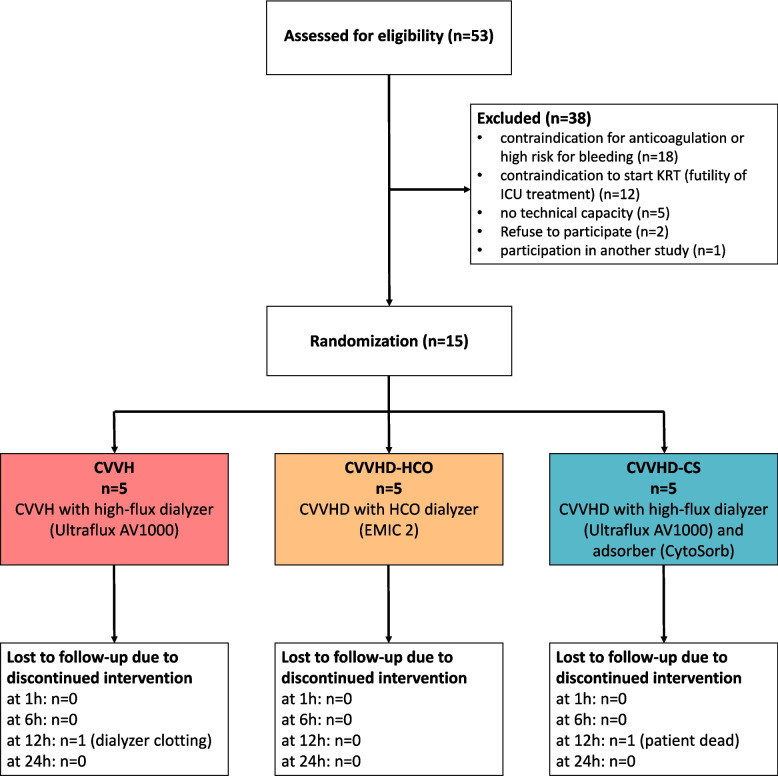
In this prospective randomized single-center study, 15 patients with rhabdomyolysis and severe AKI requiring KRT were randomized 1:1:1 into three groups: continuous veno-venous hemofiltration (CVVH), continuous veno-venous hemodialysis (CVVHD) using a high cut-off dialyzer (CVVHD-HCO), or CVVHD using a high-flux dialyzer in combination with the adsorber CytoSorb (CVVHD-CS). Concentrations of serum myoglobin, urea, creatinine, β2-microglobulin, interleukin-6, and albumin were measured before and after the dialyzer 1, 6, 12, and 24 h after initiating KRT.
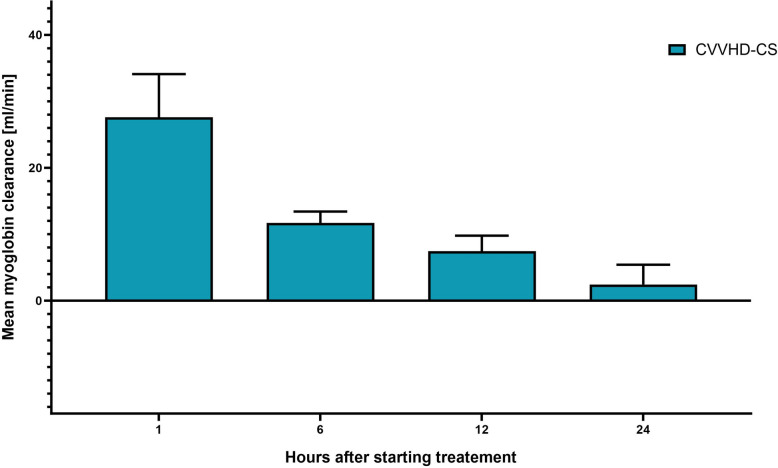
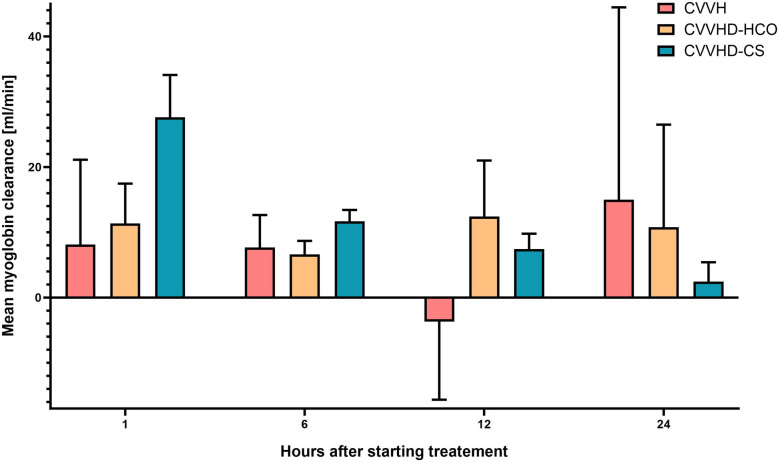
There was no significant difference in the median myoglobin clearance between the KRT modes during the 24-h study period. Nevertheless, the CVVHD-CS group showed a significantly higher myoglobin elimination compared to the other modes in the first hours of treatment. However, as a greater decline in clearance performance was observed over time, no better performance was detected over the whole study period. Simulation of different device combinations showed the highest myoglobin clearance for CVVHD-HCO combined with CS with a 12-hourly adsorber exchange interval.
All tested modes showed an effective myoglobin elimination capacity. The time-dependent elimination performance could be further increased by combining KRT with more frequent adsorber exchange.
German Clinical Trials Registry ( DRKS00023998 ); date of registration 03/03/2021.
横纹肌溶解症常与急性肾损伤(AKI)相关。由于肌红蛋白具有肾毒性,快速清除肌红蛋白至关重要。若AKI需要进行肾脏替代治疗(KRT),则应优先选择能有效清除肌红蛋白的治疗方法。本试点试验旨在比较不同的可实现肌红蛋白清除的KRT模式。
在这项前瞻性随机单中心研究中,15例患有横纹肌溶解症且因严重AKI需要进行KRT的患者被按1:1:1随机分为三组:持续性静脉-静脉血液滤过(CVVH)、使用高截留量透析器的持续性静脉-静脉血液透析(CVVHD-HCO)或使用高通量透析器联合吸附器CytoSorb的CVVHD(CVVHD-CS)。在开始KRT后1、6、12和24小时,分别于透析器前及透析器后测量血清肌红蛋白、尿素、肌酐、β2-微球蛋白、白细胞介素-6和白蛋白的浓度。
在24小时的研究期间,各KRT模式之间的肌红蛋白清除中位数无显著差异。然而,在治疗的最初几个小时内,CVVHD-CS组的肌红蛋白清除率明显高于其他模式。但随着时间推移,清除性能下降幅度更大,在整个研究期间未发现其具有更好的性能。不同设备组合的模拟显示,CVVHD-HCO联合CS且吸附器每12小时更换一次时,肌红蛋白清除率最高。
所有测试模式均显示出有效的肌红蛋白清除能力。通过更频繁地更换吸附器将KRT联合使用,可进一步提高随时间变化的清除性能。
德国临床试验注册中心(DRKS00023998);注册日期2021年3月3日。