Wang Zizhuo, Yang Tingting, Zhang Lijie, Makamure Joyman, Hong Wei, Liang Bin
Department of Radiology, Hubei Key Laboratory of Molecular Imaging, Union Hospital, Tongji Medical College, Huazhong University of Science and Technology, Wuhan, China.
J Gastrointest Oncol. 2024 Dec 31;15(6):2642-2655. doi: 10.21037/jgo-24-527. Epub 2024 Dec 28.
Hepatocellular carcinoma (HCC) patients with coronavirus disease 2019 (COVID-19) undergoing open surgery show increased adverse events (AEs) and mortality, while the safety of transarterial chemoembolization (TACE) in coinfected patients remains understudied, limiting available evidence. This study aims to investigate the safety of TACE in HCC patients coinfected with COVID-19, and to explore the potential risk factors affecting the occurrence of serious AEs (SAEs), thus providing evidence for clinical treatment strategies in such patients.
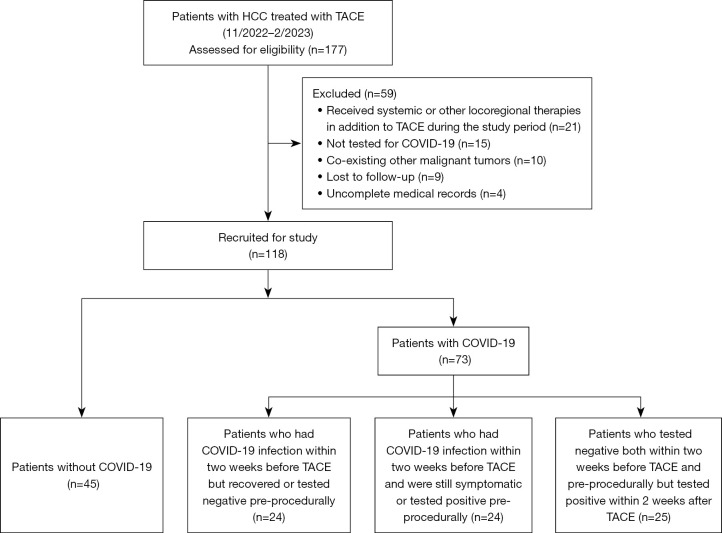
This retrospective study involved HCC patients who underwent TACE with or without COVID-19 infection at our institution from November 2022 to February 2023. Quantitative reverse transcription-polymerase chain reaction (qRT-PCR) was used for the diagnosis of COVID-19. Patients were divided into an infected group (diagnosed with COVID-19 within 2 weeks before or after the procedure) and an uninfected group (tested negative for COVID-19). SAEs were ascertained according to the National Cancer Institute Common Terminology Criteria for Adverse Events (NCI-CTCAE) version 5.0. Logistic regression analysis of multiple clinical factors in preoperative baseline characteristics was performed to identify risk factors that might predict the occurrence of SAEs.
A total of 118 patients (73 in the infected group, 45 in the uninfected group) were included, of whom 83.9% were male (86.3% in the infected group 80.0% in the uninfected group) and the median age was 55.9±12.4 years (56.8±12.3 54.5±12.7 years). The clinical spectrum of COVID-19 in the infected group were 80.8% mild, 13.7% moderate, 1.4% severe and 4.1% critical. Sixteen of the 118 patients experienced SAEs (19.2% 4.4%, P=0.046). The predominant SAEs were respiratory system diseases (9.6% 0.0%) and liver damage (2.7% 2.2%). In the univariate analysis, infection status [odds ratio (OR): 5.102, P=0.04, 95% confidence interval (CI): 1.102-23.627], gender (OR: 2.857, P=0.09, 95% CI: 0.862-9.468), age (OR: 1.061, P=0.03, 95% CI: 1.007-1.118) and clinical spectrum of COVID-19 (OR: 4.259, P<0.001, 1.943-9.336) were considered as the potential risk factors of grade ≥3 AEs. In multivariate analysis, younger age (OR: 1.064, P=0.044, 95% CI: 1.002-1.131) and a milder clinical spectrum of COVID-19 (OR: 5.736, P=0.004, 95% CI: 1.772-18.568) were independent factors associated with a lower occurrence of SAEs.
TACE in HCC patients co-infected with COVID-19 was considered relatively safe. Age and clinical spectrum of COVID-19 were associated with SAEs in HCC patients treated with TACE.
接受开放手术的2019冠状病毒病(COVID-19)合并肝细胞癌(HCC)患者不良事件(AE)和死亡率增加,而经动脉化疗栓塞术(TACE)在合并感染患者中的安全性仍研究不足,限制了现有证据。本研究旨在调查TACE在COVID-19合并HCC患者中的安全性,并探索影响严重AE(SAE)发生的潜在危险因素,从而为这类患者的临床治疗策略提供证据。
本回顾性研究纳入了2022年11月至2023年2月在我院接受或未感染COVID-19的TACE治疗的HCC患者。采用定量逆转录聚合酶链反应(qRT-PCR)诊断COVID-19。患者分为感染组(在手术前或后2周内诊断为COVID-19)和未感染组(COVID-19检测阴性)。根据美国国立癌症研究所不良事件通用术语标准(NCI-CTCAE)第5.0版确定SAE。对术前基线特征中的多个临床因素进行逻辑回归分析,以确定可能预测SAE发生的危险因素。
共纳入118例患者(感染组73例,未感染组45例),其中83.9%为男性(感染组86.3%,未感染组80.0%),中位年龄为55.9±12.4岁(感染组56.8±12.3岁,未感染组54.5±12.7岁)。感染组COVID-19的临床谱为轻症80.8%、中症13.7%、重症1.4%、危重症4.1%。118例患者中有16例发生SAE(19.2%对4.4%,P = 0.046)。主要的SAE为呼吸系统疾病(9.6%对0.0%)和肝损伤(2.7%对2.2%)。单因素分析中,感染状态[比值比(OR):5.102,P = 0.04,95%置信区间(CI):1.102 - 23.627]、性别(OR:2.857,P = 0.09,95% CI:0.862 - 9.468)、年龄(OR:1.061,P = 0.03,95% CI:1.007 - 1.118)和COVID-19临床谱(OR:4.259,P < 0.001,1.943 - 9.336)被视为≥3级AE的潜在危险因素。多因素分析中,年龄较小(OR:1.064,P = 0.044,95% CI:1.002 - 1.131)和COVID-19临床谱较轻(OR:5.736,P = 0.004,95% CI:1.772 - 18.568)是与SAE发生率较低相关的独立因素。
COVID-19合并HCC患者的TACE被认为相对安全。年龄和COVID-19临床谱与接受TACE治疗的HCC患者的SAE相关。