Kumar Sharath, Yalagudri Sachin, Saggu Daljeet, Mansoor M, Tourani Vijaya K, Narasimhan Calambur
Department of Electrophysiology, Department of Cardiology AIG Institute of Cardiac Sciences and Research Hyderabad India.
Department of Pathology Care Hospitals Hyderabad India.
J Arrhythm. 2024 Nov 14;41(1):e13181. doi: 10.1002/joa3.13181. eCollection 2025 Feb.
We present a case series of patients with granulomatous myocarditis presenting as atrial arrhythmias accompanied by lymphadenopathy.
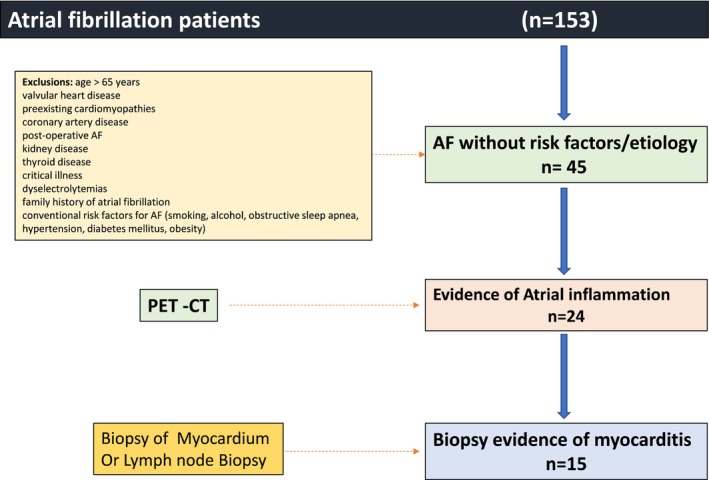
Atrial myocarditis (AM) may be the cause of atrial fibrillation (AF) in patients without risk factors.
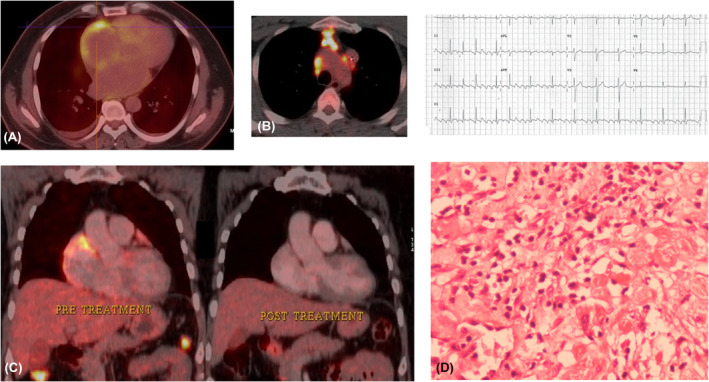
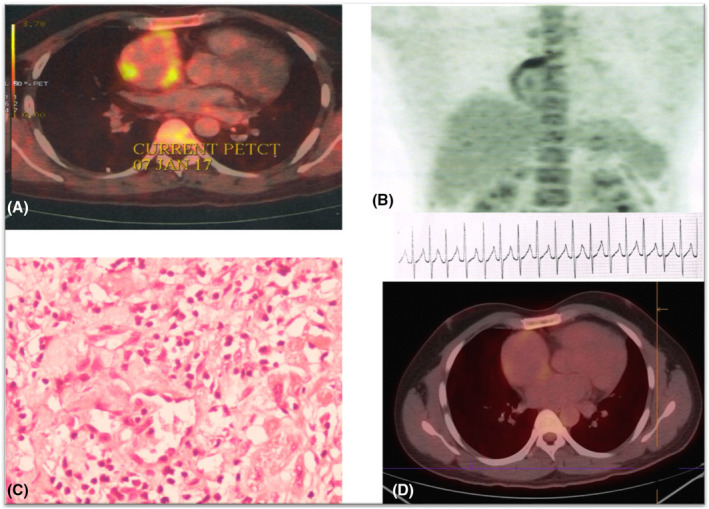
Patients with atrial fibrillation without risk factors underwent 18F-Fluorodeoxyglucose positron emission tomography (18F-FDG-PET). We performed biopsy of lymph nodes or myocardium in patients with atrial uptake of 18F-FDG-PET.
AM was observed in 15 patients. The median age of the patients was 42 years and left ventricular ejection fraction (LVEF) at presentation was 45%. All patients had AF, atrial flutter was noted in 4 patients (26.7%) and 2 patients (13.3%) had atrioventricular nodal reentrant tachycardia (AVNRT). 18F-FDG-PET uptake was noted in the atria in all patients and in the ventricles in 3 patients (20%). Cardiac sarcoidosis was the diagnosis in 12 patients (80%) while 3 patients (20%) had tuberculosis. The median CHA2DS2 VASc score was 1. Four patients (26.7%) presented with ischemic stroke. All patients were treated with disease-specific therapy in addition to antiarrhythmic medications. Over a median follow up of 26 months, a significant improvement in clinical status commensurate with a decline in atrial uptake was noted. A non-significant improvement in LVEF to 56% with disease-specific therapy was observed. ( = 0.09).
Atrial fibrillation with granulomatous lymphadenopathy may be a presenting feature of AM. The risk of stroke is high in these individuals. AM should be suspected in young individuals presenting with atrial fibrillation and stroke without conventional risk factors.
我们报告一组以房性心律失常伴淋巴结病为表现的肉芽肿性心肌炎患者病例系列。
无危险因素的患者中,心房心肌炎(AM)可能是心房颤动(AF)的病因。
无危险因素的心房颤动患者接受18F-氟脱氧葡萄糖正电子发射断层扫描(18F-FDG-PET)。对18F-FDG-PET心房摄取阳性的患者进行淋巴结或心肌活检。
15例患者诊断为AM。患者的中位年龄为42岁,就诊时左心室射血分数(LVEF)为45%。所有患者均有房颤,4例(26.7%)患者出现心房扑动,2例(13.3%)患者有房室结折返性心动过速(AVNRT)。所有患者心房均有18F-FDG-PET摄取,3例(20%)患者心室有摄取。12例(80%)患者诊断为心脏结节病,3例(20%)患者患有肺结核。CHA2DS2 VASc评分中位数为1。4例(26.7%)患者发生缺血性卒中。所有患者除抗心律失常药物外均接受了针对疾病的治疗。中位随访26个月时,临床状况有显著改善,心房摄取下降。观察到针对疾病的治疗使LVEF非显著提高至56%(P = 0.09)。
伴有肉芽肿性淋巴结病的心房颤动可能是AM的一种表现特征。这些个体发生卒中的风险较高。对于无传统危险因素而出现心房颤动和卒中的年轻个体,应怀疑AM。