Kageyama Shigetaka, Revaiah Pruthvi Chenniganahosahalli, Tsung-Ying Tsai, Miyashita Kotaro, Tobe Akihiro, O'Leary Neil, Reiber Johan H C, Tu Shengxian, Zaman Azfar, Sabaté Manel, Möllmann Helge, Sharif Faisal, Lemoine Julien, Wlodarczak Adrian, Garg Scot, Onuma Yoshinobu, Serruys Patrick W
Department of Cardiology, University of Galway, University Road, Galway, H91 TK33, Ireland.
Corrib Core Lab, University of Galway, Galway, Ireland.
Sci Rep. 2025 Jan 17;15(1):2228. doi: 10.1038/s41598-025-85872-9.
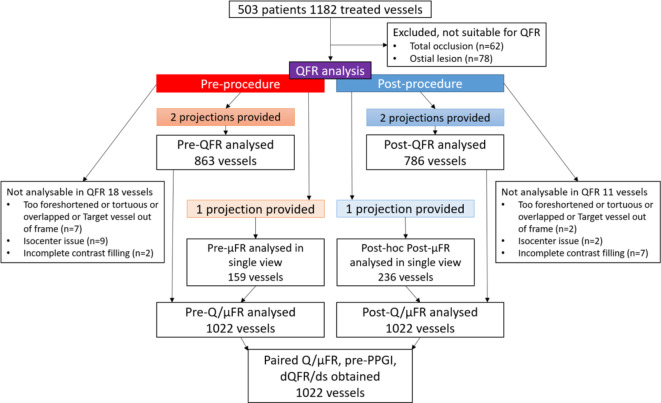
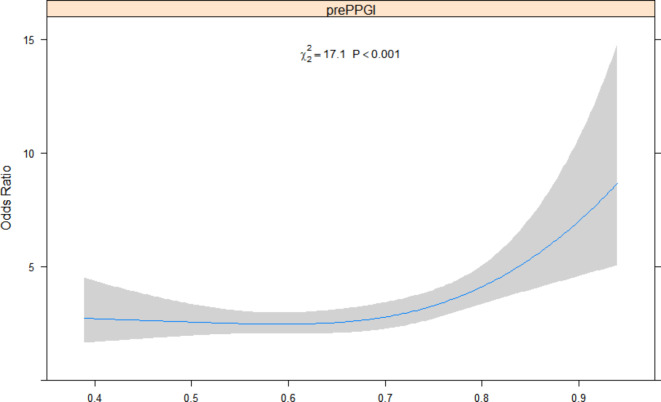
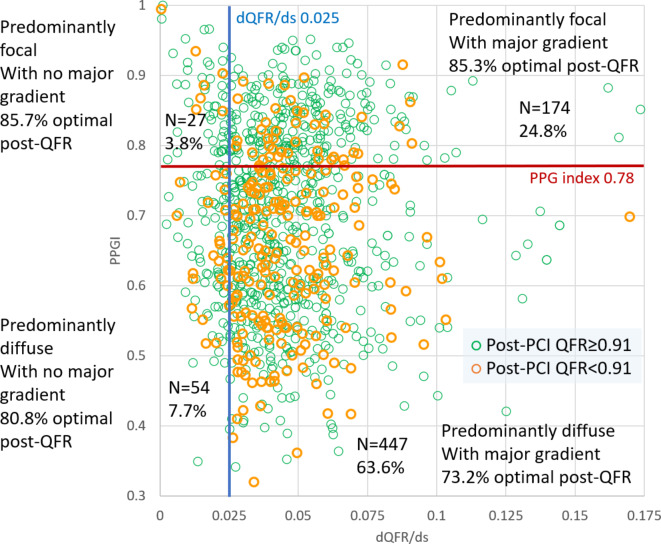
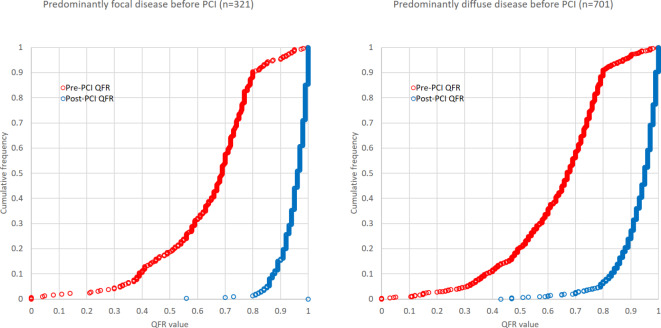
Diffuse coronary artery disease (CAD) impacts the immediate hemodynamic and clinical outcomes of percutaneous coronary intervention (PCI). We evaluated whether the diffuse pattern of CAD derived from angiographic Quantitative flow ratio (QFR) impacts the immediate hemodynamic outcome post-PCI and the medium term predicted vessel-oriented composite endpoint (VOCE). Paired pre-procedure QFRs were assessed in 503 patients and 1022 vessels in the Multivessel TALENT (MVT) trial. The pathophysiological pattern of CAD was defined as "predominantly diffuse" or "focal" according to a virtual QFR pullback pressure gradient (PPG) index < 0.78 and ≥ 0.78, respectively. Physiological "focal severity" was assessed using the QFR gradient per mm (dQFR/ds), with a value ≥ 0.025/mm the threshold for a "major gradient". A post-PCI QFR ≥ 0.91 was considered optimal. Median pre-PCI PPG index was 0.70 (IQR 0.59-0.80). The prevalence of "predominantly diffuse" CAD and "major gradient" were 68.6% and 85.8%, respectively. A "Predominantly diffuse" pattern with a major gradient had a higher risk of a post-PCI QFR < 0.91 (OR 1.52,95%CI 1.47-1.58). In multivariable analysis, low QFR PPG index (diffuse disease) was an independent determinant of a post-PCI QFR < 0.91 (per 0.1 decrease of QFR PPG index, OR:9.8, 95% CI 3.0-32.2, p < 0.001). Based on post-PCI QFR the predicted 2-year VOCE, a powered endpoint in the MVT trial, was 6.1% and 4.2% in diffuse and focal lesions, respectively. A pre-procedure physiological pattern of diffuse CAD is an independent determinant of an unfavourable immediate hemodynamic outcome post-PCI, and detrimentally affects the predicted 2-year VOCE.Clinical Trial Registration URL: https://www.clinicaltrials.gov/ct2/show/NCT04390672 Unique Identifier: NCT04390672 (registration date 15/05/2020).
弥漫性冠状动脉疾病(CAD)会影响经皮冠状动脉介入治疗(PCI)的即时血流动力学和临床结局。我们评估了源自血管造影定量血流比率(QFR)的CAD弥漫模式是否会影响PCI术后的即时血流动力学结局以及中期预测的血管导向复合终点(VOCE)。在多支血管TALENT(MVT)试验中,对503例患者和1022支血管进行了术前配对QFR评估。根据虚拟QFR回撤压力梯度(PPG)指数分别<0.78和≥0.78,将CAD的病理生理模式定义为“主要为弥漫性”或“局灶性”。使用每毫米QFR梯度(dQFR/ds)评估生理“局灶严重程度”,值≥0.025/mm为“主要梯度”阈值。PCI术后QFR≥0.91被认为是最佳的。术前PPG指数中位数为0.70(四分位间距0.59 - 0.80)。“主要为弥漫性”CAD和“主要梯度”的患病率分别为68.6%和85.8%。具有主要梯度的“主要为弥漫性”模式发生PCI术后QFR<0.91的风险更高(比值比1.52,95%置信区间1.47 - 1.58)。在多变量分析中,低QFR PPG指数(弥漫性疾病)是PCI术后QFR<0.91的独立决定因素(QFR PPG指数每降低0.1,比值比:9.8,95%置信区间3.0 - 32.2,p<0.001)。基于PCI术后QFR,MVT试验中的动力终点——预测的2年VOCE在弥漫性病变和局灶性病变中分别为6.1%和4.2%。术前弥漫性CAD的生理模式是PCI术后即时血流动力学不良结局的独立决定因素,并对预测的2年VOCE产生不利影响。临床试验注册网址:https://www.clinicaltrials.gov/ct2/show/NCT04390672 唯一标识符:NCT04390672(注册日期2020年5月15日)。