Kulasekararaj Austin, Brodsky Robert, Schrezenmeier Hubert, Griffin Morag, Röth Alexander, Piatek Caroline, Ogawa Masayo, Yu Ji, Patel Ami S, Patel Yogesh, Notaro Rosario, Usuki Kensuke, Kulagin Alexander, Gualandro Sandra, Füreder Wolfgang, Peffault de Latour Regis, Szer Jeff, Lee Jong Wook
Department of Haematological Medicine, King's College Hospital, National Institute for Health Research and Wellcome King's Clinical Research Facility and King's College London, London, UK.
Division of Hematology, Johns Hopkins Medicine, Baltimore, MD, USA.
Ann Hematol. 2025 Jan;104(1):81-94. doi: 10.1007/s00277-025-06193-5. Epub 2025 Jan 22.
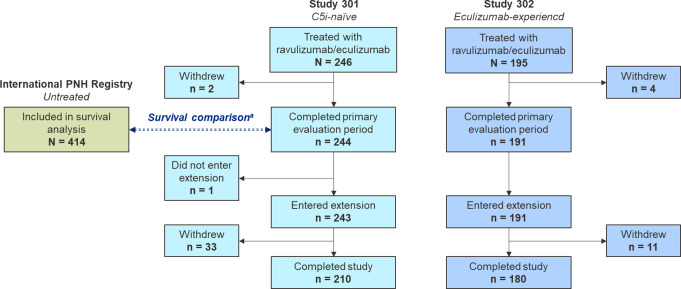
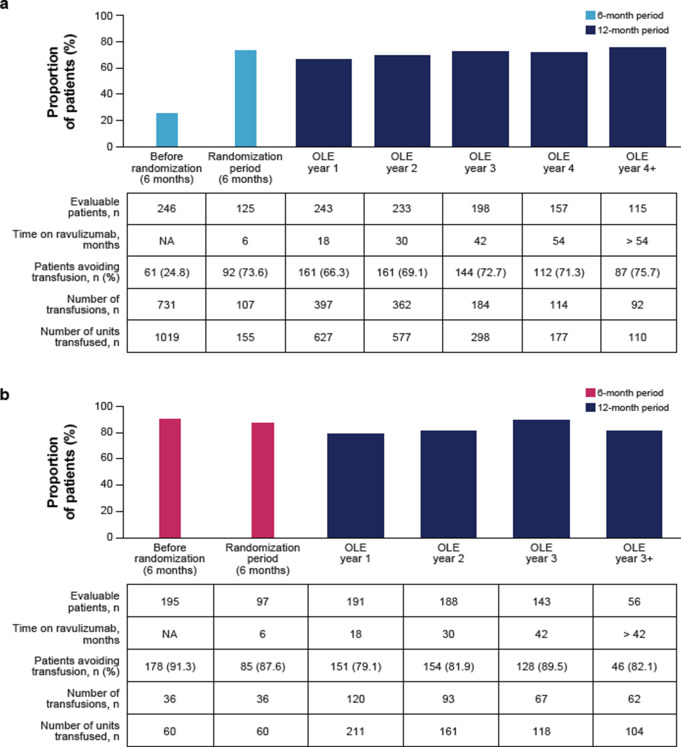
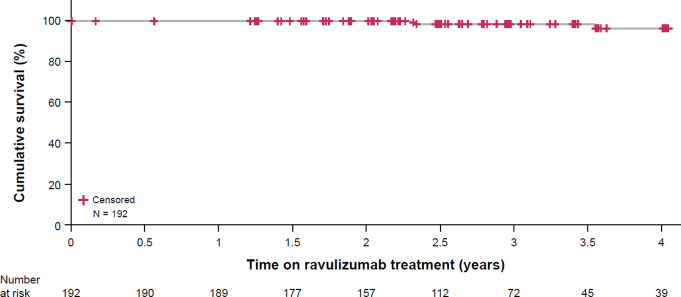
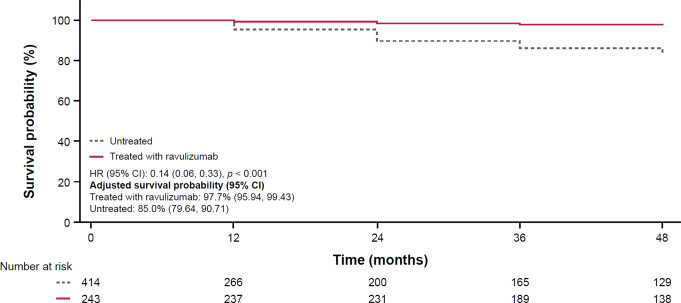
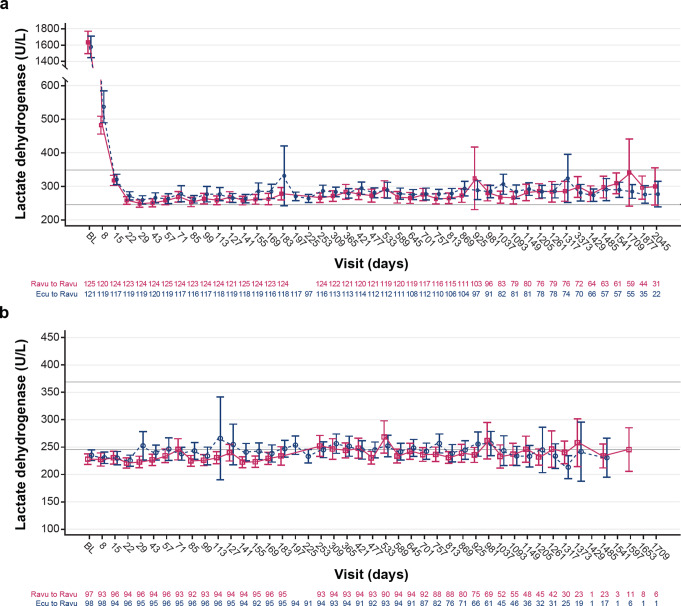
Ravulizumab is a second-generation complement component 5 (C5) inhibitor (C5i) approved for the treatment of paroxysmal nocturnal hemoglobinuria (PNH) following positive results from two pivotal trials in patients with PNH originally naive to C5i treatment and eculizumab-experienced patients with PNH. In both trials, after the 26week primary evaluation period, all patients received ravulizumab for up to 6 years. To report ravulizumab treatment outcomes in patients with PNH originally naive to C5i treatment and eculizumab-experienced patients with PNH treated for up to 6 years. Originally C5i-naive (N = 244) and eculizumab-experienced (N = 191) patients with PNH continued ravulizumab treatment for up to 6 years. Major adverse vascular events (MAVEs; including thrombotic events [TEs]) and survival are reported, including a comparison of survival with untreated patients from the International PNH Registry. Laboratory parameters for intravascular hemolysis (IVH) are also described. For up to 6 years (1468.0 patient-years of exposure), ravulizumab provided durable control of terminal complement activity and IVH, resulting in a low incidence of MAVEs (including TEs) reported (MAVE rate: 0.7-1.4 per 100 patient-years) and, compared with untreated patients from the International PNH Registry, reduced the risk of mortality by five-fold. The few breakthrough IVH events reported (N = 122) were commonly associated with complement-amplifying conditions, and only two events (1.8%) were associated with suboptimal inhibition of C5 (i.e. serum free C5 ≥ 0.5 µg/mL). These results support the long-term use of ravulizumab as the first-line treatment of choice for patients with PNH. Trial registration details: NCT01374360; registered: October 29, 2004; NCT02946463; registered: October 27, 2016; NCT03056040; registered: June 05, 2017.
ravulizumab是一种第二代补体成分5(C5)抑制剂(C5i),在两项关键试验取得阳性结果后获批用于治疗阵发性睡眠性血红蛋白尿(PNH),这两项试验的对象分别是最初未接受过C5i治疗的PNH患者以及曾使用依库珠单抗治疗过的PNH患者。在这两项试验中,经过26周的初步评估期后,所有患者均接受了长达6年的ravulizumab治疗。目的是报告最初未接受过C5i治疗的PNH患者以及曾使用依库珠单抗治疗过的PNH患者接受长达6年ravulizumab治疗的结果。最初未使用过C5i(N = 244)以及曾使用依库珠单抗治疗过(N = 191)的PNH患者继续接受了长达6年的ravulizumab治疗。报告了主要不良血管事件(MAVE,包括血栓形成事件[TE])和生存率,包括与国际PNH注册中心未治疗患者的生存率比较。还描述了血管内溶血(IVH)的实验室参数。在长达6年(1468.0患者-年的暴露时间)内,ravulizumab对终末补体活性和IVH提供了持久控制,导致报告的MAVE(包括TE)发生率较低(MAVE发生率:每100患者-年0.7 - 1.4次),并且与国际PNH注册中心未治疗患者相比,将死亡风险降低了五倍。报告的少数突破性IVH事件(N = 122)通常与补体放大情况相关,仅有两起事件(1.8%)与C5抑制不足(即血清游离C5≥0.5µg/mL)相关。这些结果支持将ravulizumab长期用作PNH患者的一线首选治疗药物。试验注册详情:NCT01374360;注册时间:2004年10月29日;NCT02946463;注册时间:2016年10月27日;NCT03056040;注册时间:2017年6月5日。