Cullari Matias Leonardo, Taleb Juan Pablo, Gutierrez Lucio, Aguirre Facundo Martín, Aguer Santiago Alejandro, Lloyd Ruy, Ernst Glenda
Orthopedic Surgery British Hospital of Buenos Aires, Buenos Aires, Argentina.
Scientific Advisory Board, Hospital Británico de Buenos Aires, Buenos Aires, Argentina.
Arch Bone Jt Surg. 2024;12(11):779-788. doi: 10.22038/ABJS.2024.79458.3637.
Investigate the immediate resonance magnetic image changes undergone by the lumbar canal after indirect decompression and compare them at one-year post-intervention. We also investigate the clinical outcome of indirect decompression at one-year follow-up.
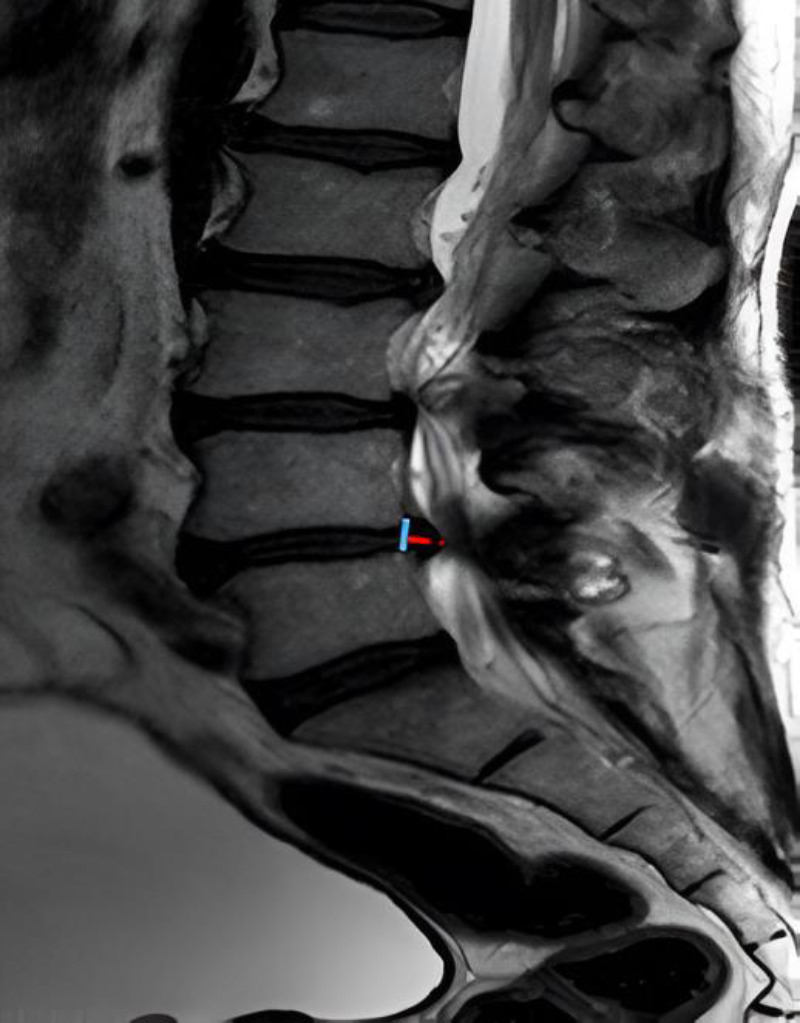
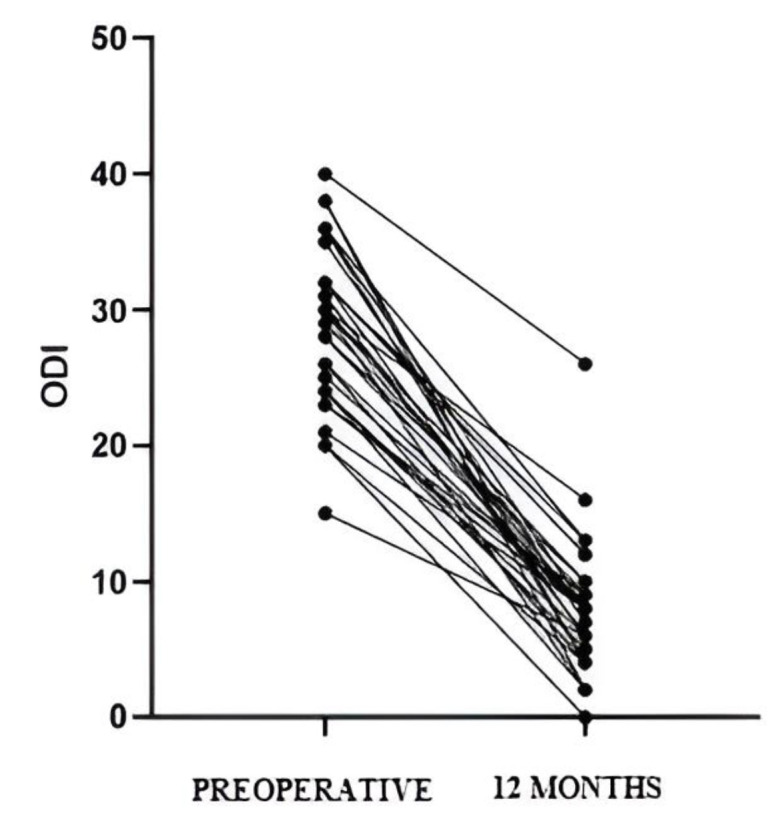
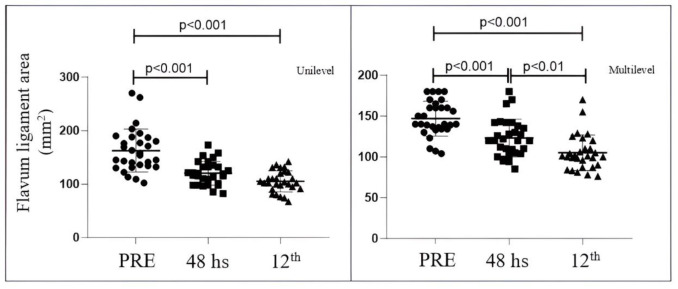
Imaging changes in patients who underwent indirect lumbar decompression and percutaneous posterior fixation were analyzed with one-year follow-up. Radiographic measurements were performed preoperatively and postoperatively (at one year), and the area of lumbar canal occupation and yellow ligament by nuclear magnetic resonance was compared preoperatively, at 48 hours post-surgery, and at one year. Radiographic measurements included disc height, foraminal height, total lumbar lordosis, and segmental lordosis. The VAS lumbar and lower limb scales and the Oswestry Disability Index (ODI) were used to assess clinical outcomes.
A total of 21 male and 23 female patients underwent indirect decompression at 64 lumbar levels. A significant improvement was observed in the clinical evaluation of all patients' post-surgery (p < 0.001) in all radiographic parameters. There was an immediate increase in the lumbar canal at 48 hours (p < 0.001), which continued to increase at one year post-intervention (p < 0.05). The yellow ligament occupation area decreased at 48 hours (p < 0.001) and continued to decrease until one year (p < 0.01). Four complications were recorded, one of which was a posterior tract infection requiring open decompression.
Indirect decompression for degenerative lumbar disease provided successful clinical outcomes, including indirect expansion of the dural sac at 48 hours post-procedure, with progressive increase in the lumbar canal area at one-year follow-up.
研究间接减压后腰椎管的即时磁共振成像变化,并在干预后一年进行比较。我们还在一年随访时研究间接减压的临床结果。
对接受间接腰椎减压和经皮后路固定的患者进行一年随访,分析其影像学变化。在术前和术后(一年时)进行影像学测量,比较术前、术后48小时和一年时磁共振成像测量的腰椎管占位面积和黄韧带面积。影像学测量包括椎间盘高度、椎间孔高度、腰椎总前凸和节段性前凸。采用视觉模拟评分法(VAS)评估腰部和下肢情况,并用Oswestry功能障碍指数(ODI)评估临床结果。
共有21例男性和23例女性患者在64个腰椎节段接受了间接减压。所有患者术后的所有影像学参数临床评估均有显著改善(p<0.001)。术后48小时腰椎管立即增大(p<0.001),干预后一年持续增大(p<0.05)。黄韧带占位面积在术后48小时减小(p<0.001),并持续减小至一年(p<0.01)。记录到4例并发症,其中1例为后路感染,需行开放减压。
退行性腰椎疾病的间接减压提供了成功的临床结果,包括术后48小时硬脊膜囊间接扩张,一年随访时腰椎管面积逐渐增加。