Stoll Felicitas, Amato Salvatore, Sauter Max, Burhenne Jürgen, Weiss Johanna, Haefeli Walter E, Blank Antje
Medical Faculty Heidelberg, Heidelberg University, 69117 Heidelberg, Germany.
Internal Medicine IX-Department of Clinical Pharmacology and Pharmacoepidemiology, Heidelberg University Hospital, 69120 Heidelberg, Germany.
Pharmaceutics. 2025 Jan 3;17(1):60. doi: 10.3390/pharmaceutics17010060.
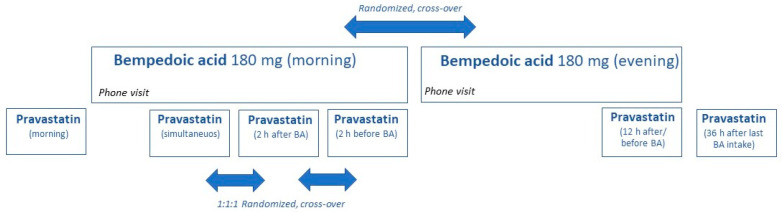
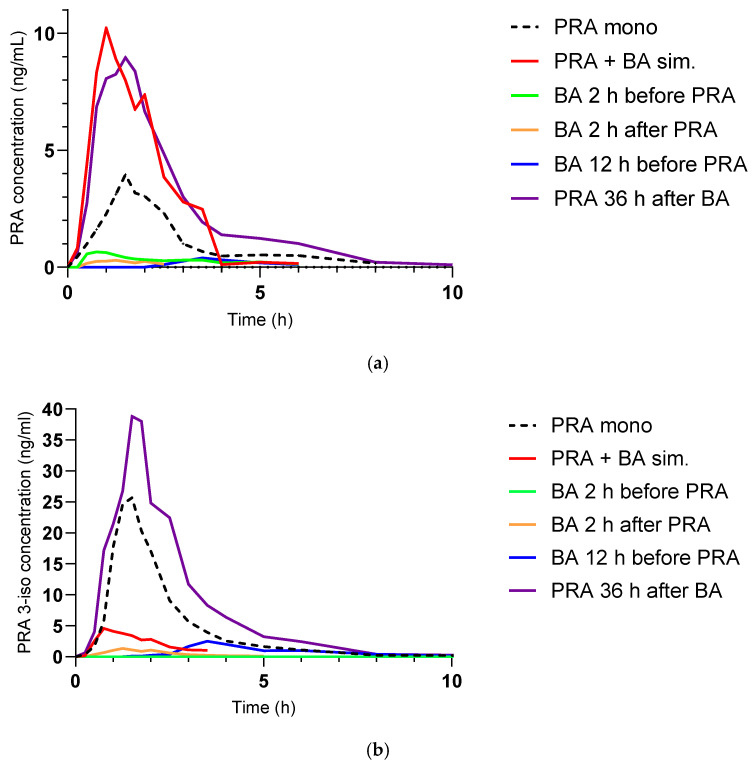
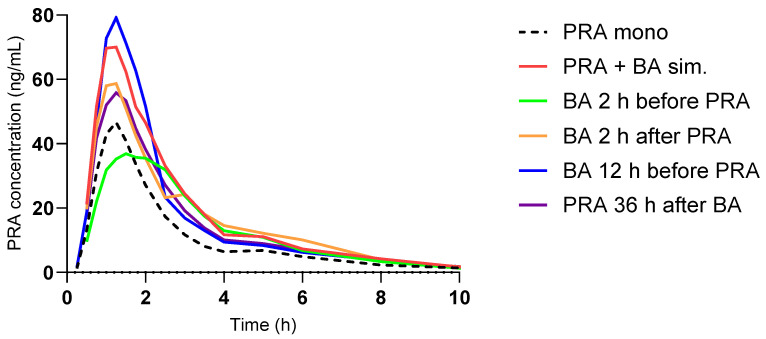
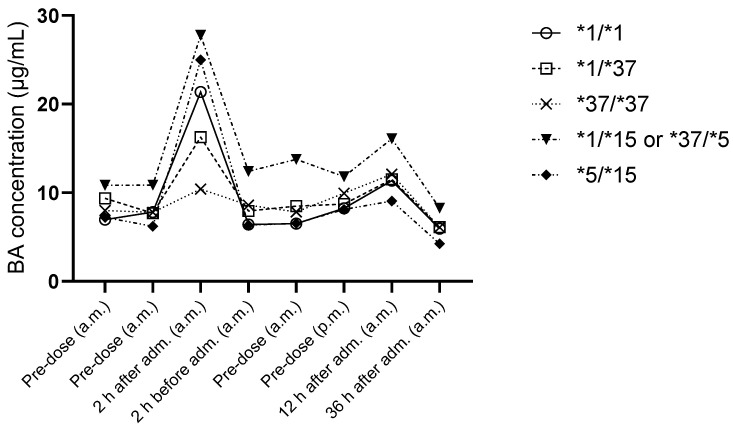
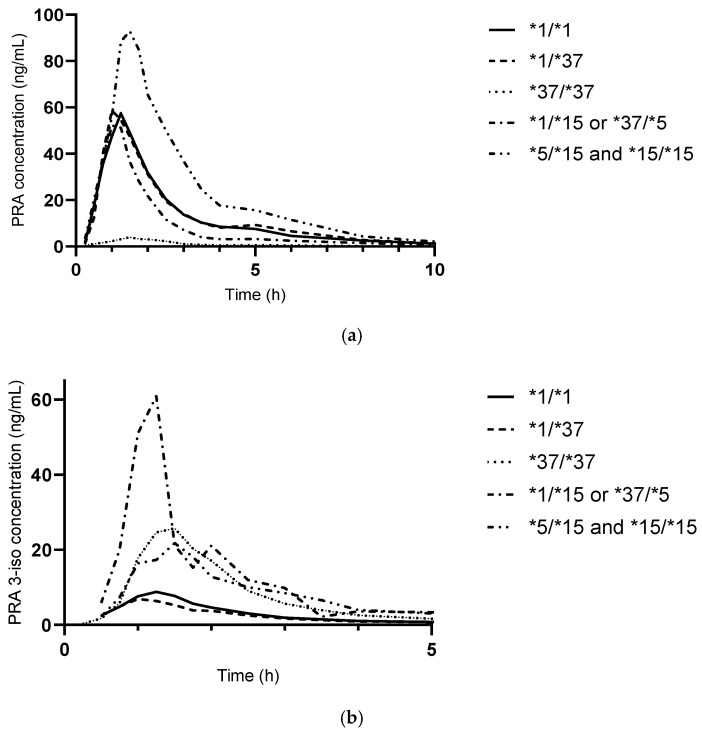
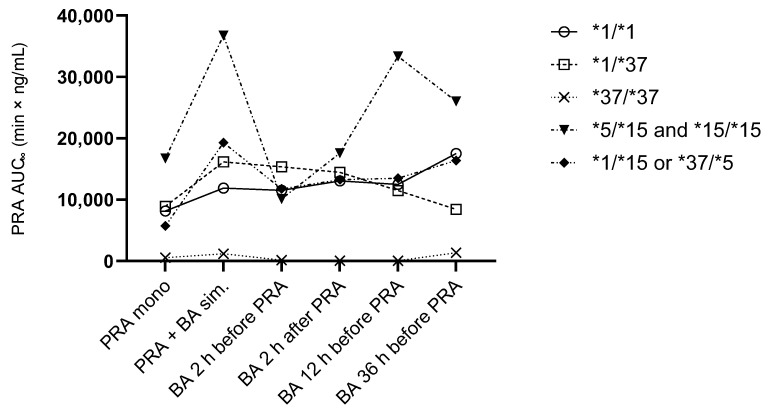
: Bempedoic acid (BA) is a novel cholesterol-lowering agent with proven positive effects on cardiovascular endpoints. Because it is an inhibitor of the hepatic transporters OATP1B1 and OATP1B3, two uptake transporters regulating the intrahepatic availability of statins, it increases the systemic exposure of co-administered statins. This interaction could raise the risk of myopathy. We hypothesized that the drug interaction between BA and statins could be mitigated by staggered administration. : This was a single-centre, open-label, randomized, two-arm, cross-over, phase I drug interaction trial in healthy volunteers (EudraCT-No: 2022-001096-13). The primary objective was to evaluate the OATP1B1 inhibitory effect of BA on exposure to pravastatin after simultaneous administration versus different schedules of staggered administration. A secondary objective was to evaluate the impact of genotypes (*1, *5, *15, *37) on pravastatin exposure. Pravastatin was administered in single oral doses of 40 mg at six visits. After a baseline visit with pravastatin alone, BA was dosed to steady state at the approved oral dose of 180 mg. Outcome measures were the area under the plasma concentration-time curve, extrapolated to infinity (AUC) and C of pravastatin, 3α-hydroxy-pravastatin (pravastatin 3-iso), and pravastatin lactone, and their geometric mean ratios (GMRs) of different schedules of administration. Log-transformed AUC and C were compared with one-way ANOVA with a 90% confidence interval (CI). : Fourteen participants completed all visits. At BA steady state, the GMRs of pravastatin AUC and C were 1.80 (90% CI 1.31-2.46) and 1.95 (90% CI 1.40-2.72), respectively, compared to baseline. There was no significant difference in pravastatin exposure between simultaneous vs. staggered administration. There was no statistically significant difference in pravastatin 3-iso or pravastatin lactone between different administration modes. For the AUC of pravastatin and pravastatin 3-iso, haplotype was a significant source of variation (63% and 20%, respectively), while the type of administration (simultaneous vs. staggered) had no significant impact. : The increase in pravastatin exposure with concomitant intake of BA was larger than expected. There was no significant difference between simultaneous vs. staggered administration of pravastatin and BA, possibly due to a population that was heterogenous in haplotypes.
贝派地酸(BA)是一种新型降胆固醇药物,已证实对心血管终点具有积极作用。由于它是肝脏转运体OATP1B1和OATP1B3的抑制剂,这两种摄取转运体调节他汀类药物的肝内可用性,因此它会增加同时服用的他汀类药物的全身暴露量。这种相互作用可能会增加肌病风险。我们假设BA与他汀类药物之间的药物相互作用可以通过错开给药来减轻。
这是一项在健康志愿者中进行的单中心、开放标签、随机、双臂、交叉的I期药物相互作用试验(欧盟临床试验编号:2022-001096-13)。主要目的是评估BA在同时给药与不同错开给药方案后对普伐他汀暴露的OATP1B1抑制作用。次要目的是评估基因型(*1、*5、*15、*37)对普伐他汀暴露的影响。在六次访视中,普伐他汀以40mg的单次口服剂量给药。在单独服用普伐他汀的基线访视后,BA以180mg的批准口服剂量给药至稳态。观察指标是血浆浓度-时间曲线下面积,外推至无穷大(AUC)以及普伐他汀、3α-羟基普伐他汀(普伐他汀3-异构体)和普伐他汀内酯的C,以及不同给药方案的几何平均比值(GMRs)。对经对数转换的AUC和C进行单因素方差分析,并给出90%置信区间(CI)。
14名参与者完成了所有访视。在BA达到稳态时,与基线相比,普伐他汀AUC和C的GMRs分别为1.80(90%CI 1.31-2.46)和1.95(90%CI 1.40-2.72)。同时给药与错开给药之间普伐他汀暴露无显著差异。不同给药方式之间普伐他汀3-异构体或普伐他汀内酯无统计学显著差异。对于普伐他汀和普伐他汀3-异构体的AUC,单倍型是一个显著的变异来源(分别为63%和2