Stylianidi Maria Chara, Vaghiri Sascha, Pandkhahi Alireza, Kazziha Sultan, Al Akeel Ward, Knoefel Wolfram Trudo, Prassas Dimitrios
Department of Surgery (A), Medical Faculty and University Hospital Duesseldorf, Heinrich-Heine-University, Moorenstr. 5, 40225, Duesseldorf, Germany.
Medical Research School Duesseldorf, Heinrich-Heine-University Duesseldorf, Moorenstr. 5, 40225, Duesseldorf, Germany.
Langenbecks Arch Surg. 2025 Jan 25;410(1):50. doi: 10.1007/s00423-025-03611-0.
The primary objective was to compare the intra- and postoperative outcomes of diaphragmatic stripping versus full-thickness diaphragmatic resection in patients with peritoneal carcinomatosis who underwent cytoreductive surgery.
According to the PRSIMA guidelines, a comprehensive literature search was conducted for studies comparing postoperative pulmonary complications as well as intra- and postoperative outcomes of diaphragmatic stripping versus full-thickness diaphragmatic resection in patients with peritoneal carcinomatosis necessitating cytoreductive surgery. Data from eligible studies were extracted, qualitatively assessed, and included in a meta-analysis. Odds ratios (ORs) and standardized mean differences (SMDs) with 95 per cent confidence intervals were calculated.
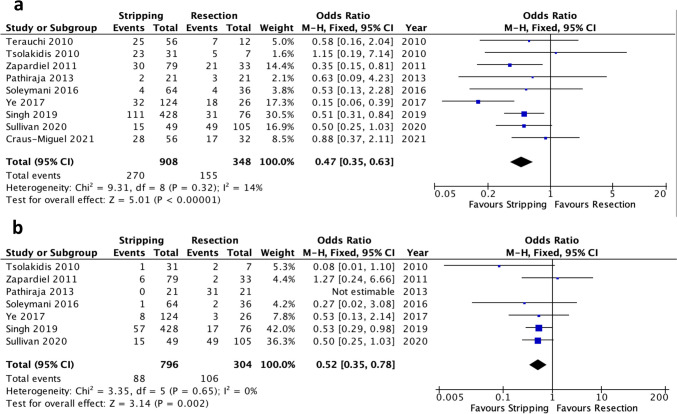
Ten studies with 1325 patients were included in this meta-analysis. Diaphragmatic stripping was associated with lower incidence of pleural effusion (OR 0.47, 95% CI 0.35-0.63, p < 0.00001) and pneumothorax (OR 0.52, 95% CI 0.35-0.78, p = 0.002), less severe postoperative complications (Clavien-Dindo Grade ≥ 3) (OR 0.43, 95% CI 0.30-0.63, p < 0.0001), and shorter duration of surgery (SMD -0.31, 95% CI -0.54 - -0.08, p = 0.007). No significant differences were observed in postoperative subdiaphragmatic abscess occurrence, intraoperative blood loss, hospital- and ICU-stay, and 90-day mortality.
Diaphragmatic stripping leads to a significantly lower rate of postoperative pulmonary and severe complications compared to diaphragmatic full-thickness resection, while oncological outcomes do not appear to be worse. Larger trials with standardized study protocols and long-term survival data are needed to validate the results presented here.
主要目的是比较接受减瘤手术的腹膜癌患者行膈肌剥脱术与膈肌全层切除术的术中和术后结果。
根据PRISMA指南,对比较术后肺部并发症以及膈肌剥脱术与膈肌全层切除术在需要减瘤手术的腹膜癌患者中的术中和术后结果的研究进行了全面的文献检索。提取符合条件的研究数据,进行定性评估,并纳入荟萃分析。计算了95%置信区间的比值比(OR)和标准化均数差(SMD)。
本荟萃分析纳入了10项研究,共1325例患者。膈肌剥脱术与较低的胸腔积液发生率(OR 0.47,95%CI 0.35 - 0.63,p < 0.00001)和气胸发生率(OR 0.52,95%CI 0.35 - 0.78,p = 0.002)相关,术后并发症较轻(Clavien-Dindo分级≥3级)(OR 0.43,95%CI 0.30 - 0.63,p < 0.0001),手术时间较短(SMD -0.31,95%CI -0.54 - -0.08,p = 0.007)。在术后膈下脓肿发生率、术中失血量、住院和ICU停留时间以及90天死亡率方面未观察到显著差异。
与膈肌全层切除术相比,膈肌剥脱术导致术后肺部和严重并发症的发生率显著降低,而肿瘤学结果似乎并不更差。需要更大规模的试验,采用标准化的研究方案和长期生存数据来验证此处呈现的结果。