Wu Jing, Liu Yuqing, Wang Chuncheng, Liu Lianjie, Lu Jiaqian
School of Public Administration, Yanshan University, No. 438 West Hebei Avenue, Qinhuangdao, 066004, China.
Department of Gastroenterology, First Hospital of Qinhuangdao, No. 258 Wenhua Road, Qinhuangdao, 066000, China.
BMC Health Serv Res. 2025 Jan 25;25(1):145. doi: 10.1186/s12913-025-12304-9.
To address the health inequity caused by decentralized management, China has introduced a provincial pooling system for urban employees' basic medical insurance. This paper proposes a research framework to evaluate similar policies in different contexts. This paper adopts a mixed-methods approach to more comprehensively and precisely capture the causal effects of the policy. Ultimately, this paper aims to assess the impact of the UPA policy on health inequity.
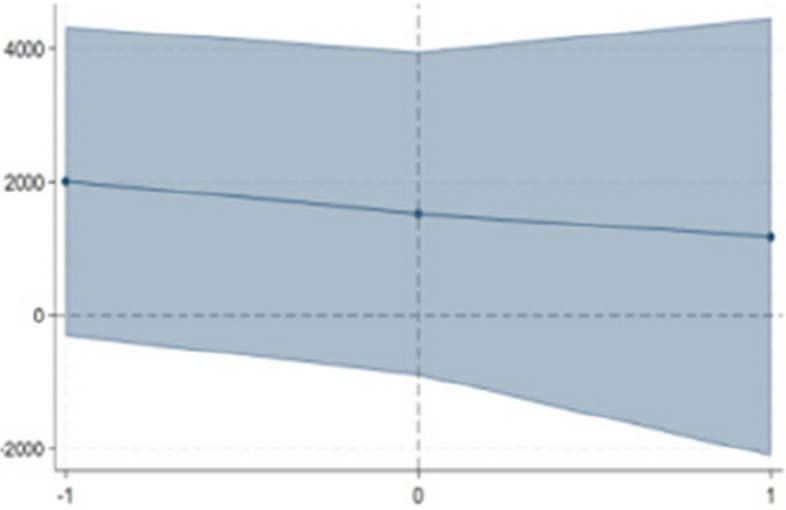
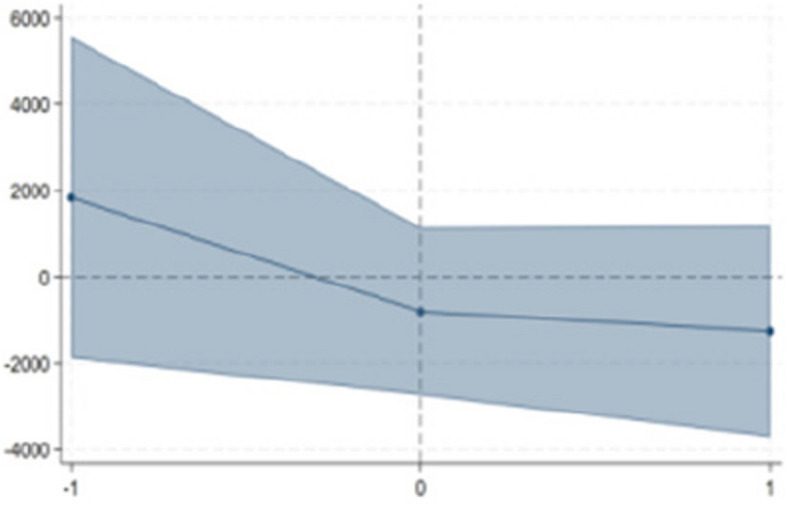
This study takes the provincial unified reform of basic medical insurance for urban employees in China as an example, uses the China Family Panel Studies (CFPS) data and related policy documents, and adopts the DID-RIF hybrid method to test the impact of the equalization of the medical insurance system on health inequity, by using the interaction term in the DID (Difference-in-Differences) model as the independent variable in the RIF (Recentered Influence Function) to exclude the influence of other interfering variables. In addition, the DID method explores the effects of UPA on medical expenditures, which can guide the improvement of the policy.
The empirical results show that the UPA policy increases the likelihood of patients developing chronic diseases within six months. Although factors such as age, gender, and marital status influence the probability of chronic disease, health inequity between income groups after the policy's implementation primarily stems from the rise in outpatient and reimbursement expenses.
Although the gap in medical reimbursement expenses between participants of different socioeconomic statuses narrowed after the provincial medical insurance pooling reform, health inequity among the insured population increased. The equalized health insurance reform failed to address health inequities based on socioeconomic status. Additionally, the reverse reallocation of medical resources and outpatient arbitrage driven by moral hazard warrant close attention. This paper recommends that, in advancing the provincial pooling of UEBMI, greater focus should be placed on strengthening digital oversight and improving the hierarchical diagnosis and treatment system to promote social equity.
为解决分散管理导致的健康不平等问题,中国推出了城镇职工基本医疗保险省级统筹制度。本文提出了一个研究框架,以评估不同背景下的类似政策。本文采用混合方法,更全面、精确地捕捉政策的因果效应。最终,本文旨在评估省级统筹政策对健康不平等的影响。
本研究以中国城镇职工基本医疗保险省级统一改革为例,利用中国家庭追踪调查(CFPS)数据及相关政策文件,采用双重差分-重新中心化影响函数(DID-RIF)混合方法,通过将双重差分(DID)模型中的交互项作为重新中心化影响函数(RIF)中的自变量,来检验医疗保险制度均等化对健康不平等的影响,以排除其他干扰变量的影响。此外,双重差分法探究省级统筹对医疗支出的影响,可为政策改进提供指导。
实证结果表明,省级统筹政策增加了患者在六个月内患慢性病的可能性。尽管年龄、性别和婚姻状况等因素会影响患慢性病的概率,但政策实施后不同收入群体之间的健康不平等主要源于门诊和报销费用的增加。
尽管省级医疗保险统筹改革后,不同社会经济地位参与者之间医疗报销费用的差距有所缩小,但参保人群中的健康不平等却有所增加。均等化的医疗保险改革未能解决基于社会经济地位的健康不平等问题。此外,由道德风险驱动的医疗资源反向配置和门诊套利值得密切关注。本文建议,在推进城镇职工基本医疗保险省级统筹时,应更加注重加强数字化监管,完善分级诊疗制度,以促进社会公平。