Takeno Kenichi, Sugano Motoki, Kokubo Yasuo
Department of Orthopaedic Surgery, Sugita Genpaku Memorial Obama Municipal Hospital, Fukui, Japan.
Department of General Surgery, Sugita Genpaku Memorial Obama Municipal Hospital, Fukui, Japan.
AME Case Rep. 2024 Nov 27;9:29. doi: 10.21037/acr-24-128. eCollection 2025.
Open pelvic fractures are rare but represent a serious clinical problem with high mortality rates. Acute mortality is often associated with hemorrhage, whereas delayed mortality is most often associated with sepsis and multiple organ failure. We report a case of Wang's classification of type II open pelvic ring fracture with hemorrhagic shock and septic shock from gas gangrene.
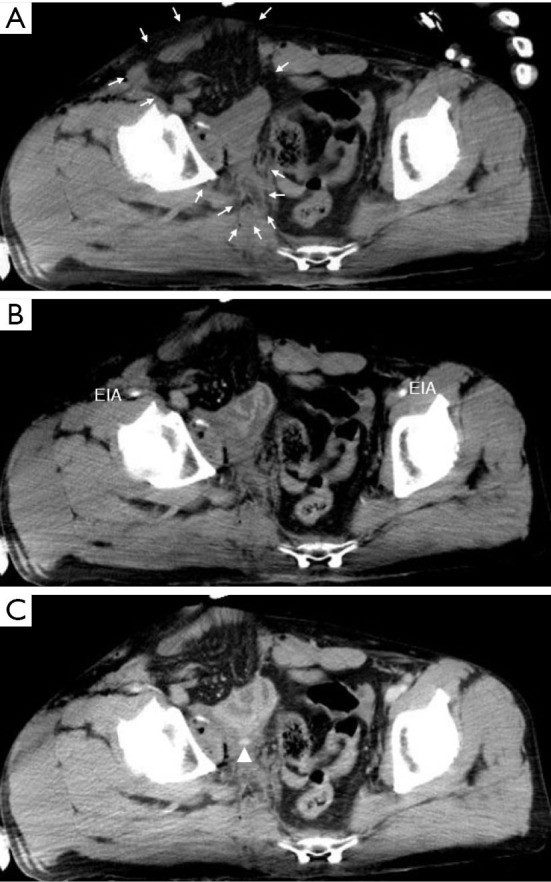
A healthy 41-year-old man presented with an open pelvic ring fracture and a laceration in the lower abdomen sustained at an ironworks. His hemodynamic status was unstable. Pelvic ring stabilization with an external fixator, ligation of the median sacral and bilateral internal iliac arteries, partial resection of the ileum, appendectomy, and intra-abdominal pelvic packing were performed. Seven days after the injury, he developed a single spike fever of 39.8 ℃ with a significant pus discharge from the open wound around his groin. A computed tomography scan revealed an accumulation of gas around the sacroiliac joint, in the abdominal cavity, and the adductors and gluteus maximus muscles caused by non-clostridial gas gangrene. We performed surgical debridement three times and initiated vancomycin administration. Hyperbaric oxygen therapy was also initiated as an adjunctive therapy. The patient could walk with a cane 5 months after the injury.
We described a multidisciplinary case of a patient with a Wang type II open pelvic fracture who required emergent damage control and subsequently developed anaerobic sepsis. Bleeding was controlled by packing gauze into the intraperitoneal cavity and applying external fixation to the pelvic ring. However, it is important to administer prophylactic antibiotics against anaerobic bacteria and to detect subsequent infections early when packing gauze into the intraperitoneal cavity in patients with open pelvic fractures.
开放性骨盆骨折较为罕见,但却是一个严重的临床问题,死亡率很高。急性死亡率通常与出血有关,而延迟性死亡率最常与脓毒症和多器官功能衰竭有关。我们报告一例王氏分类法中的II型开放性骨盆环骨折病例,该患者同时发生出血性休克和气性坏疽性感染性休克。
一名41岁健康男性,在一家钢铁厂受伤,出现开放性骨盆环骨折和下腹部撕裂伤。他的血流动力学状态不稳定。进行了外固定架固定骨盆环、结扎骶中动脉和双侧髂内动脉、部分切除回肠、阑尾切除术以及腹腔盆腔填塞术。受伤7天后,他出现一次体温高达39.8℃的发热,腹股沟周围开放伤口有大量脓性分泌物。计算机断层扫描显示,由非产气荚膜梭菌性气性坏疽导致骶髂关节周围、腹腔内以及内收肌和臀大肌有气体积聚。我们进行了三次手术清创,并开始使用万古霉素。还启动了高压氧治疗作为辅助治疗。受伤5个月后,患者可以拄拐行走。
我们描述了一例王氏II型开放性骨盆骨折患者的多学科治疗病例,该患者需要紧急损伤控制,随后发生厌氧性脓毒症。通过向腹腔内填塞纱布和对骨盆环进行外固定来控制出血。然而,对于开放性骨盆骨折患者,在向腹腔内填塞纱布时,预防性使用抗厌氧菌抗生素并早期检测后续感染非常重要。