Bun Krufinta, Mode Benedict, Susapu Melinda, Salo Joyceline, Bjerum Catherine, Payne Michael, Tisch Daniel, Sekihara Makoto, Giorgi Emanuele, Weil Gary J, Fischer Peter U, Robinson Leanne, Laman Moses, King Christopher L
Department of Pathology, Center for Global Health and Disease, Case Western Reserve University, Cleveland, Ohio, United States of America.
Provincial Health Department, Kokopo, East New Britain Province, Papua New Guinea.
PLoS Negl Trop Dis. 2025 Jan 27;19(1):e0012128. doi: 10.1371/journal.pntd.0012128. eCollection 2025 Jan.
WHO recommends two annual rounds of mass drug administration (MDA) with ivermectin, diethylcarbamazine, and albendazole (IDA) for lymphatic filariasis (LF) elimination in treatment naïve areas that are not co-endemic for onchocerciasis such as Papua New Guinea (PNG). Whether two rounds of MDA are necessary or sufficient and the optimal sampling strategies and endpoints for stopping MDA remain undefined.
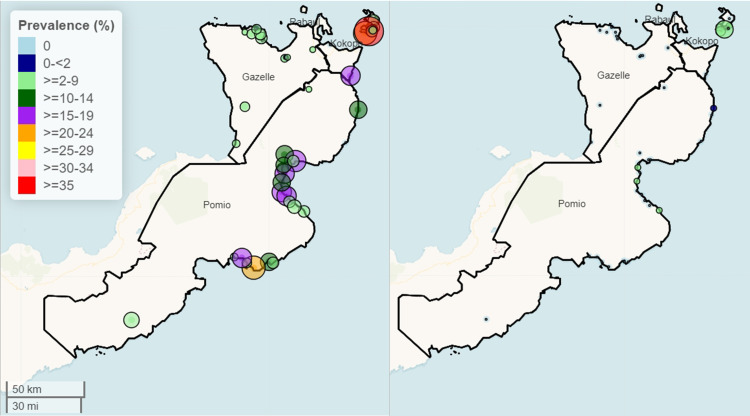
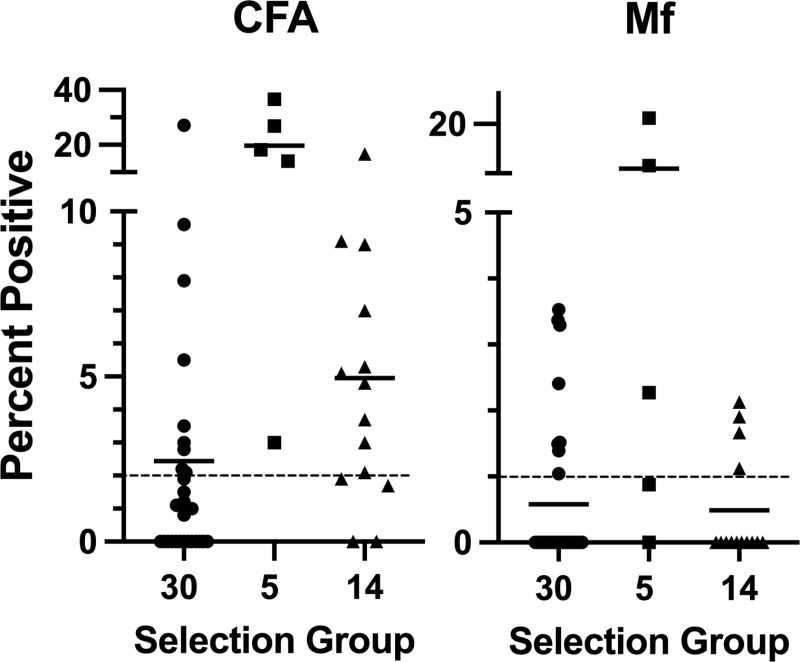
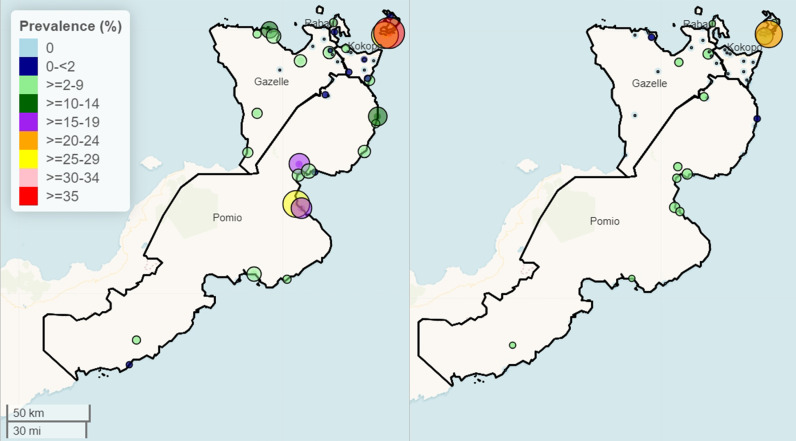
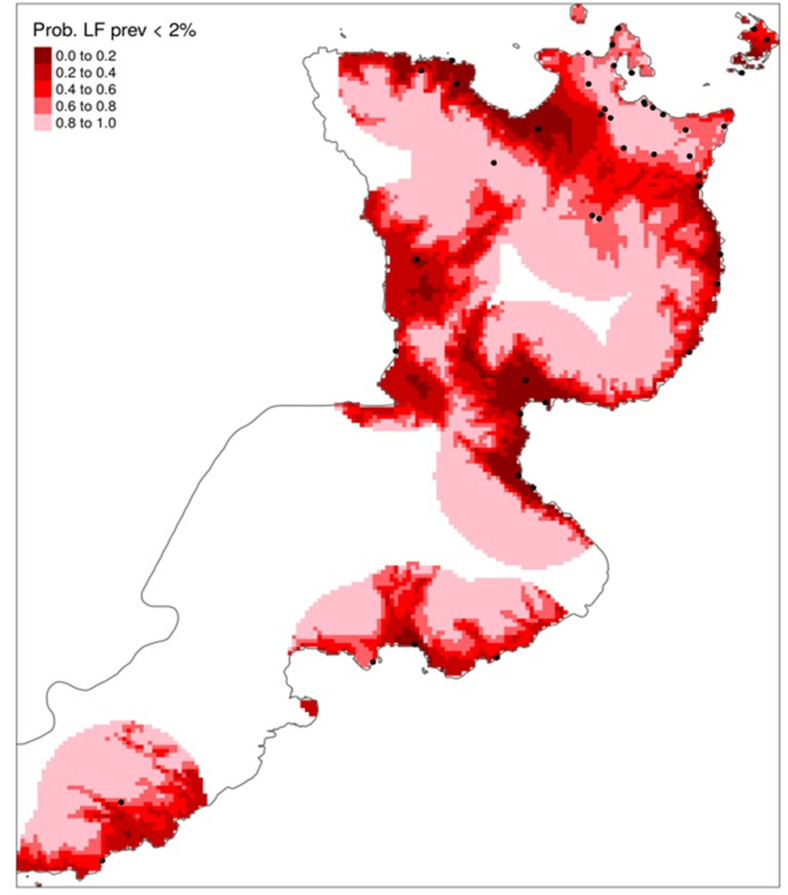
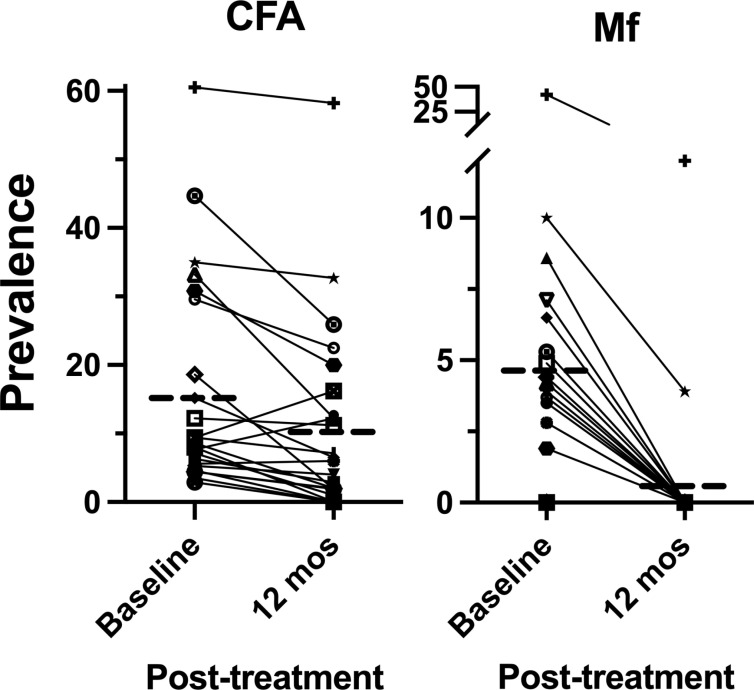
Two cross-sectional studies were conducted at baseline (N = 49 clusters or villages) and 12 months after mass drug administration (MDA) with IDA (N = 47 villages) to assess lymphatic filariasis (LF) by circulating filarial antigenemia (CFA) and microfilariae (Mf). Before MDA, children aged 6-9 years (N50) and those ≥ 10 years (N50) in each village were randomly sampled. Before MDA, the population mean prevalence of LF in East New Britain Province (ENBP), Papua New Guinea, was estimated using population proportionate sampling (PPS, N = 30) to be 59/2,561 (2.3%) CFA positive and 14/2,561 (0.6%) Mf positive. No children were Mf positive. However, LF infection was highly heterogeneous; 8 villages (26.7%) had a CFA prevalence >2%, and 7 villages (23.3%) had an Mf prevalence >1%. To identify sentinel villages with LF in areas under-sampled by PPS, 19 additional villages suspected to have LF were sampled, with 15 (79%) having >2% CFA prevalence and 7 (38%) >1% Mf (range 1-22%). Twenty-four villages were evaluated before and after MDA in age-matched adults ( ≥ 18 years). Treatment reduced CFA prevalence by 34% and Mf prevalence by 90%. Post-MDA model-based geostatistics efficiently selected an additional 23 villages, of which 20 (87%) had a CFA prevalence > 2%. None of these villages had >1% Mf. Post-MDA, two of four districts had no villages with >1% Mf.
Model-based geostatistics was more effective than PPS in sampling high-risk LF sites in a heterogeneous area. Low LF prevalence and partial reduction of CFA limit children's effectiveness as sentinels. A single round of high-coverage MDA with IDA achieved elimination targets in low-prevalence villages in PNG. Higher-prevalence areas will need additional MDA rounds, which could be targeted to smaller evaluation units to cut costs.
Clinicaltrials.gov NCT04124250.
世界卫生组织建议,对于巴布亚新几内亚(PNG)等未同时流行盘尾丝虫病的未接受过治疗地区,每年进行两轮使用伊维菌素、乙胺嗪和阿苯达唑(IDA)的大规模药物给药(MDA)以消除淋巴丝虫病(LF)。两轮MDA是否必要或足够,以及停止MDA的最佳抽样策略和终点仍不明确。
在基线时(N = 49个群组或村庄)以及使用IDA进行大规模药物给药(MDA)后12个月(N = 47个村庄)进行了两项横断面研究,通过循环丝虫抗原血症(CFA)和微丝蚴(Mf)评估淋巴丝虫病(LF)。在MDA之前,每个村庄随机抽取6至9岁(N50)和≥10岁(N50)的儿童。在MDA之前,使用按人口比例抽样(PPS,N = 30)估计巴布亚新几内亚东新不列颠省(ENBP)LF的总体患病率为59/2,561(2.3%)CFA阳性和14/2,561(0.6%)Mf阳性。没有儿童Mf阳性。然而,LF感染高度异质性;8个村庄(26.7%)CFA患病率>2%,7个村庄(23.3%)Mf患病率>1%。为了在PPS抽样不足的地区识别有LF的哨点村庄,另外抽取了19个疑似有LF的村庄,其中15个(79%)CFA患病率>2%,7个(38%)Mf患病率>1%(范围为1 - 22%)。对24个村庄的年龄匹配成年人(≥18岁)在MDA前后进行了评估。治疗使CFA患病率降低了34%,Mf患病率降低了90%。基于MDA后模型的地统计学有效地选择了另外23个村庄,其中20个(87%)CFA患病率>2%。这些村庄中没有一个Mf患病率>1%。MDA后,四个区中有两个区没有Mf患病率>1%的村庄。
在异质地区抽样高风险LF地点时,基于模型的地统计学比PPS更有效。LF患病率低和CFA部分降低限制了儿童作为哨点的有效性。一轮高覆盖率的IDA MDA在PNG的低患病率村庄实现了消除目标。患病率较高的地区将需要额外的MDA轮次,可针对较小的评估单位以降低成本。
Clinicaltrials.gov NCT04124250。