Eastern and Southern Africa Centre of International Parasite Control, Kenya Medical Research Institute, Nairobi, Kenya.
Department of Epidemiology, Statistics and Informatics, Kenya Medical Research Institute, Nairobi, Kenya.
PLoS Negl Trop Dis. 2024 Jul 8;18(7):e0011942. doi: 10.1371/journal.pntd.0011942. eCollection 2024 Jul.
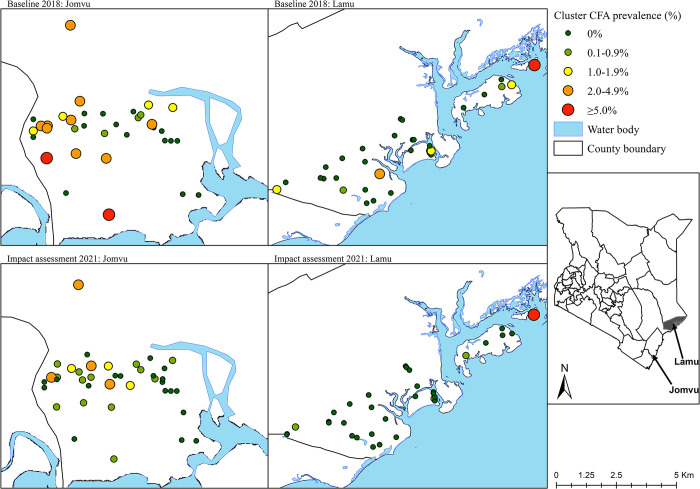
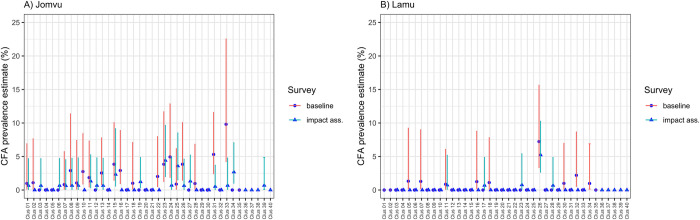
The World Health Organization (WHO) endorsed the use of triple-drug mass drug administration (MDA) regimen with ivermectin, diethylcarbamazine (DEC) and albendazole (commonly abbreviated as IDA) to accelerate the elimination of lymphatic filariasis (LF) as a public health problem in settings where onchocerciasis is not co-endemic. The National Programme for Elimination of LF (NPELF) in Kenya was among the first adopters of the IDA-MDA and two annual rounds were provided in 2018 and 2019 to the residents of Lamu County and Jomvu sub-County in the coast region. This study documented the feasibility of successfully delivering the two rounds of IDA-MDA. An operational research study was undertaken to determine efficient sampling strategies, indicators, and the appropriate population groups that could be used for the monitoring and evaluation of LF programs using IDA-MDA for the elimination of the disease as a public health problem. Two cross-sectional surveys were conducted at baseline in 2018 before IDA-MDA and an impact assessment 17 months after the second round of IDA-MDA. The reported epidemiological treatment coverage was at least 80% in all implementation units during each round of IDA-MDA. Blood samples were tested for filarial antigenemia using commercial Filariasis Test Strips (FTS) and any individual found to be positive was tested again at night for the presence of microfilariae in finger prick blood smears using microscopy. The overall prevalence of circulating filarial antigen (CFA) was relatively low at the baseline survey with Jomvu having 1.39% (95% CI: 0.91, 2.11) and Lamu having 0.48% (95% CI: 0.21, 1.13). Significant reduction in CFA prevalence was observed during the impact assessment after the two annual rounds of mass treatment. The overall relative reduction (%) in CFA prevalence following the two rounds of MDA with IDA was significant in both Jomvu (52.45%, Z = -2.46, P < 0.02) and Lamu (52.71%, Z = -1.97, P < 0.05). Heterogeneity, however, was observed in the CFA prevalence reduction between random and purposive clusters, as well as between adult and child populations. The results of the impact assessment survey offered strong evidence that it was safe to stop the IDA-MDA in the two EUs because transmission appears to have been interrupted. It is also important to implement a post-treatment surveillance system which would enable efficient detection of any recrudescence of LF transmission at a sub-evaluation unit level. Our findings show that IDA-MDA may be considered for acceleration of LF elimination in other settings where onchocerciasis is not co-endemic.
世界卫生组织(WHO)支持使用伊维菌素、乙胺嗪和阿苯达唑(简称 IDA)的三药大规模药物治疗(MDA)方案,以加速消除淋巴丝虫病(LF)作为一个公共卫生问题,在盘尾丝虫病非共患地区。肯尼亚国家淋巴丝虫病消除规划(NPELF)是首批采用 IDA-MDA 的机构之一,2018 年和 2019 年向沿海地区拉穆县和乔姆武县的居民提供了两轮治疗。本研究记录了成功开展两轮 IDA-MDA 的可行性。进行了一项业务研究,以确定有效的抽样策略、指标以及可用于监测和评估使用 IDA-MDA 消除 LF 作为一个公共卫生问题的规划的适当人群。在 IDA-MDA 之前的 2018 年基线进行了两项横断面调查,并在第二轮 IDA-MDA 后 17 个月进行了影响评估。在每一轮 IDA-MDA 中,所有实施单位的报告流行病学治疗覆盖率至少为 80%。使用商业丝虫病检测试剂盒(FTS)检测血液中的丝虫抗原血症,对任何检测呈阳性的个体,再次在夜间用手指刺破血液涂片进行显微镜检查,检测微丝蚴的存在。基线调查中循环丝状抗原(CFA)的总体流行率相对较低,乔姆武为 1.39%(95%CI:0.91,2.11),拉穆为 0.48%(95%CI:0.21,1.13)。在两轮大规模治疗后的影响评估中,CFA 流行率显著下降。在两轮 IDA-MDA 治疗后,CFA 流行率的总体相对下降(%)在乔姆武(52.45%,Z=-2.46,P<0.02)和拉穆(52.71%,Z=-1.97,P<0.05)均有统计学意义。然而,在随机和定向聚类之间以及成人和儿童人群之间,CFA 流行率的降低存在异质性。影响评估调查的结果提供了强有力的证据,表明在这两个 EUs 停止 IDA-MDA 是安全的,因为传播似乎已经中断。实施治疗后监测系统也很重要,这将能够在亚评估单位层面有效检测 LF 传播的任何复燃。我们的研究结果表明,在盘尾丝虫病非共患地区,IDA-MDA 可考虑用于加速 LF 消除。