Gao Aili, Tian Xin, Lang Dexiu, Chen Yue
Department of Dermatology, Guangzhou Dermatology Hospital, Guangzhou, Guangdong, People's Republic of China.
Clin Cosmet Investig Dermatol. 2025 Jan 21;18:201-206. doi: 10.2147/CCID.S492503. eCollection 2025.
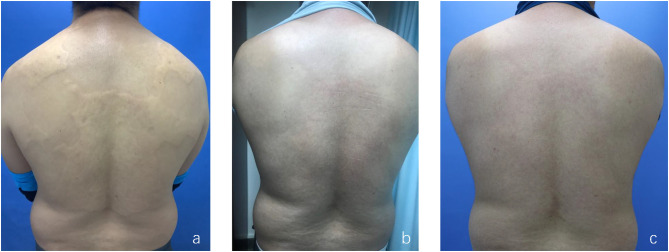
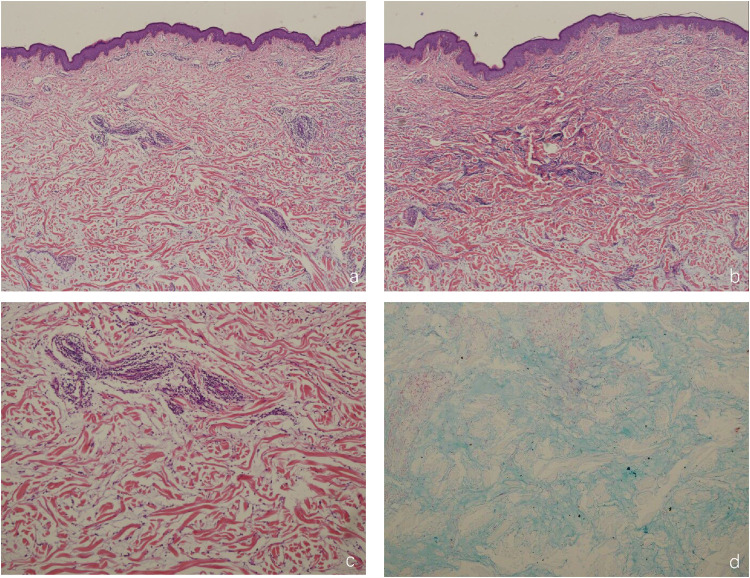
Scleromyxedema (SM) is a rare primary cutaneous mucinosis characterized by systemic papules and scleroderma-like manifestations, often associated with monoclonal gammopathy. We present the case of a 37-year-old male with SM who developed yellowish plaques on the neck and back over three years. Histopathological examination revealed mucin deposition, fibroblast proliferation, and fibrosis, supporting the diagnosis. Serum protein electrophoresis identified IgG-λ type paraproteinemia. Notably, the patient had a history of hepatitis B virus (HBV) infection, suggesting a potential association. Following eight weeks of oral triamcinolone acetonide therapy, the skin lesions improved significantly. Despite established diagnostic criteria for SM, its pathogenesis remains poorly understood. Chronic antigenic stimulation from circulating cytokines and viral infections, such as HBV, may contribute to disease development. This case highlights the potential link between chronic HBV infection and SM, emphasizing the need for further investigation into viral etiologies. SM differs clinically, histologically, and systemically from related disorders such as scleroderma and scleroedema, necessitating careful differentiation for appropriate management. The scarcity of epidemiological data and lack of standardized treatment guidelines for SM in China underscore the challenges clinicians face in diagnosing and managing this rare disease. This case reinforces the importance of multidisciplinary collaboration, particularly when co-infections such as HBV are present. Given the chronic, unpredictable course of SM and its potential systemic involvement, continuous follow-up and vigilant monitoring are essential to optimize patient outcomes.
硬化性黏液水肿(SM)是一种罕见的原发性皮肤黏蛋白病,其特征为全身性丘疹和硬皮病样表现,常与单克隆丙种球蛋白病相关。我们报告一例37岁患有SM的男性患者,其颈部和背部出现淡黄色斑块已达三年之久。组织病理学检查显示有黏蛋白沉积、成纤维细胞增殖和纤维化,支持该诊断。血清蛋白电泳确定为IgG-λ型副蛋白血症。值得注意的是,该患者有乙型肝炎病毒(HBV)感染史,提示可能存在关联。口服曲安奈德治疗八周后,皮肤病变明显改善。尽管有既定的SM诊断标准,但其发病机制仍知之甚少。循环细胞因子和病毒感染(如HBV)引起的慢性抗原刺激可能促使疾病发展。该病例突出了慢性HBV感染与SM之间的潜在联系,强调需要进一步调查病毒病因。SM在临床、组织学和全身表现上与硬皮病和硬化性水肿等相关疾病不同,需要仔细鉴别以进行适当管理。中国SM的流行病学数据匮乏且缺乏标准化治疗指南,凸显了临床医生在诊断和管理这种罕见疾病时面临的挑战。该病例强化了多学科协作的重要性,尤其是在存在HBV等合并感染的情况下。鉴于SM病程慢性、不可预测且可能累及全身,持续随访和密切监测对于优化患者预后至关重要。