Johnston Brian W, Downes Michael, Hall Angela, Thomas Zachary, Welters Ingeborg D
Department of Cardiovascular and Metabolic Medicine, Faculty of Health and Life Sciences, Institute of Life Course and Medical Sciences, University of Liverpool, Liverpool, United Kingdom.
Liverpool University Hospitals NHS Foundation Trust, Liverpool, United Kingdom.
PLoS One. 2025 Jan 29;20(1):e0318365. doi: 10.1371/journal.pone.0318365. eCollection 2025.
New Onset Atrial Fibrillation (NOAF) is the most common arrhythmia in intensive care. Complications of NOAF include thromboembolic events such as myocardial infarction and stroke, which contribute to a greater risk of mortality. Inflammatory and coagulation biomarkers in sepsis are thought to be associated with NOAF development. The aim of this systematic review and narrative synthesis is to identify inflammatory and coagulation biomarkers as predisposing risk factors for NOAF in sepsis.
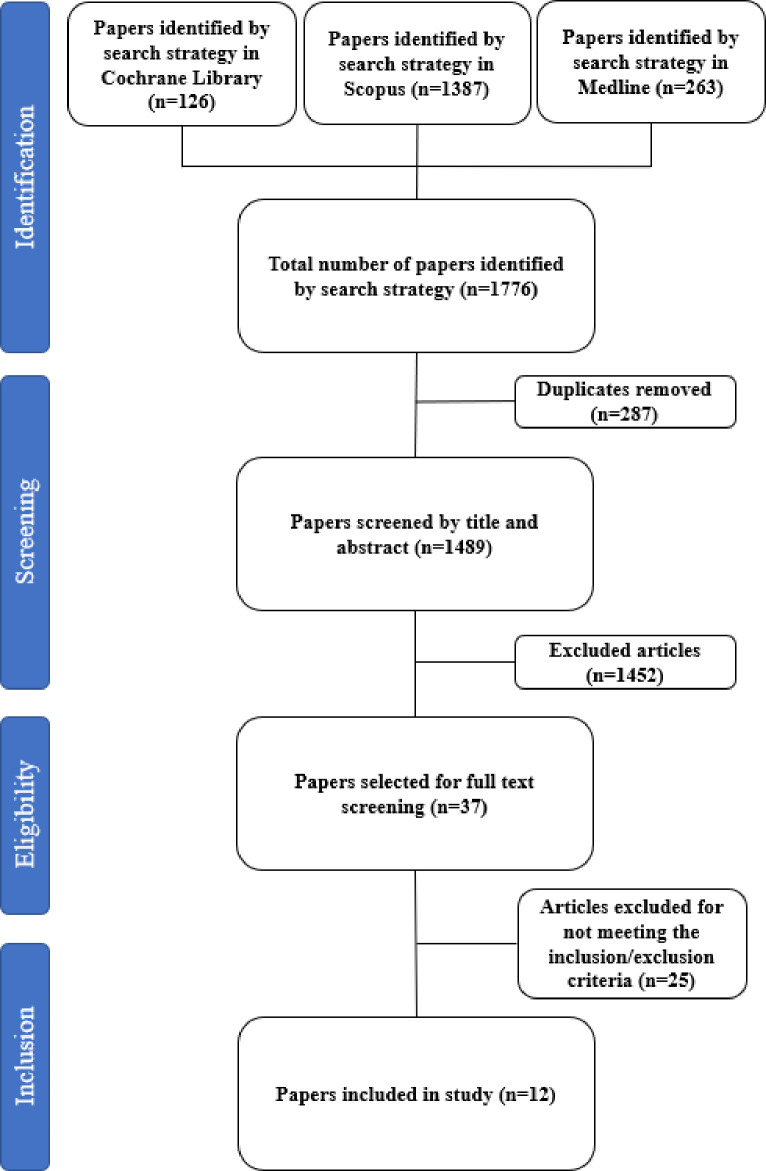
Three databases (Medline, Cochrane Library, and Scopus) were searched using a predefined search strategy. Inclusion / exclusion criteria were applied, and quality assessments were performed using the Newcastle Ottawa Scale (NOS).
We identified 1776 articles; and 12 articles were included in this review. 8 articles were retrospective observational studies and 4 were prospective observational studies. There was considerable heterogeneity between studies regarding outcomes, methodological design, quality, definitions and reported biomarkers of interest. There is evidence that C-reactive protein (CRP) is associated with NOAF, with hazard ratios 3.33 (3.32-3.35) p = 0.001 and odds ratios of 1.011 (1.008-1.014) p<0.001. International Normalised Ratio (INR) and fibrinogen may be associated with NOAF with odds ratios reported as 1.837 (1.270-2.656) p = 0.001 and 1.535(1.232-1.914) p<0.001 respectively.
Further research is required to confirm the association between inflammatory and coagulation biomarkers and the development of NOAF in sepsis. A broader evidence base will guide treatment strategies, improving the standard of care for patients who develop NOAF in sepsis. Furthermore, given the heterogeneity between studies consideration should be given to inclusion of immune biomarkers in future core outcome sets for trials investigating NOAF.
新发房颤(NOAF)是重症监护中最常见的心律失常。NOAF的并发症包括血栓栓塞事件,如心肌梗死和中风,这会增加死亡风险。脓毒症中的炎症和凝血生物标志物被认为与NOAF的发生有关。本系统评价和叙述性综合分析的目的是确定炎症和凝血生物标志物作为脓毒症中NOAF的易感风险因素。
使用预定义的检索策略检索三个数据库(Medline、Cochrane图书馆和Scopus)。应用纳入/排除标准,并使用纽卡斯尔渥太华量表(NOS)进行质量评估。
我们共检索到1776篇文章;本综述纳入了12篇文章。8篇为回顾性观察性研究,4篇为前瞻性观察性研究。在研究结果、方法设计、质量、定义和报告的相关生物标志物方面,各研究之间存在相当大的异质性。有证据表明,C反应蛋白(CRP)与NOAF相关,风险比为3.33(3.32 - 3.35),p = 0.001,比值比为1.011(1.008 - 1.014),p < 0.001。国际标准化比值(INR)和纤维蛋白原可能与NOAF相关,比值比分别报告为1.837(1.270 - 2.656),p = 0.001和1.535(1.232 - 1.914),p < 0.001。
需要进一步研究以证实炎症和凝血生物标志物与脓毒症中NOAF发生之间的关联。更广泛的证据基础将指导治疗策略,提高脓毒症中发生NOAF患者的护理标准。此外,鉴于各研究之间的异质性,在未来调查NOAF的试验核心结局集中应考虑纳入免疫生物标志物。