Debatisse Justine, Chalet Lucie, Eker Omer Faruk, Cho Tae-Hee, Becker Guillaume, Wateau Océane, Wiart Marlène, Costes Nicolas, Mérida Inés, Léon Christelle, Langlois Jean-Baptiste, Lancelot Sophie, Lux François, Boutelier Timothé, Nighoghossian Norbert, Mechtouff Laura, Canet-Soulas Emmanuelle
Université Claude Bernard Lyon1, CarMeN Laboratory, INSERM, INRAE, Bât. B13, Groupement Hospitalier Est, 59 Boulevard Pinel, Lyon, France.
Université Claude Bernard Lyon1, CarMeN Laboratory, INSERM, INRAE, Bât. B13, Groupement Hospitalier Est, 59 Boulevard Pinel, Lyon, France; Olea Medical, La Ciotat, France.
Neurotherapeutics. 2025 Mar;22(2):e00529. doi: 10.1016/j.neurot.2025.e00529. Epub 2025 Jan 31.
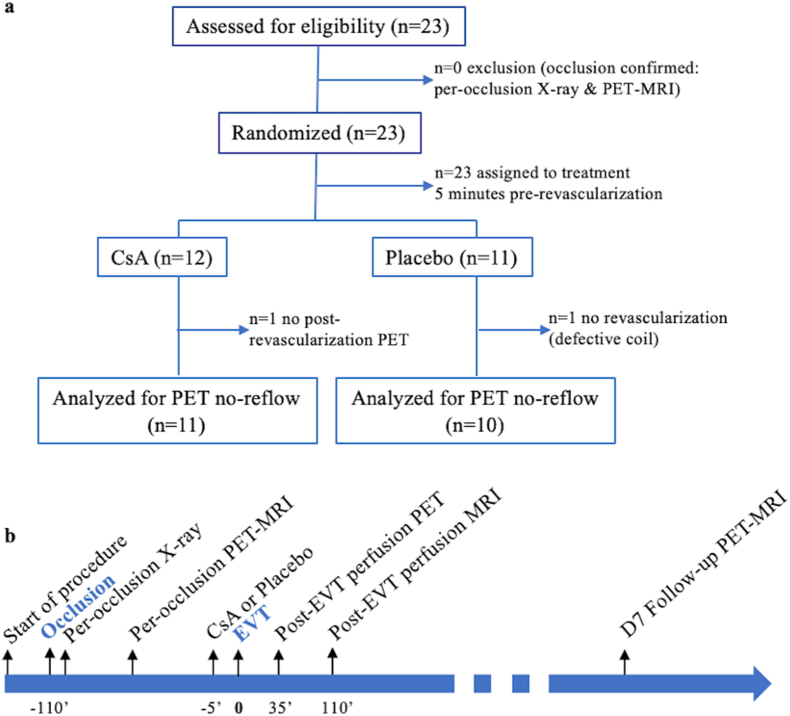
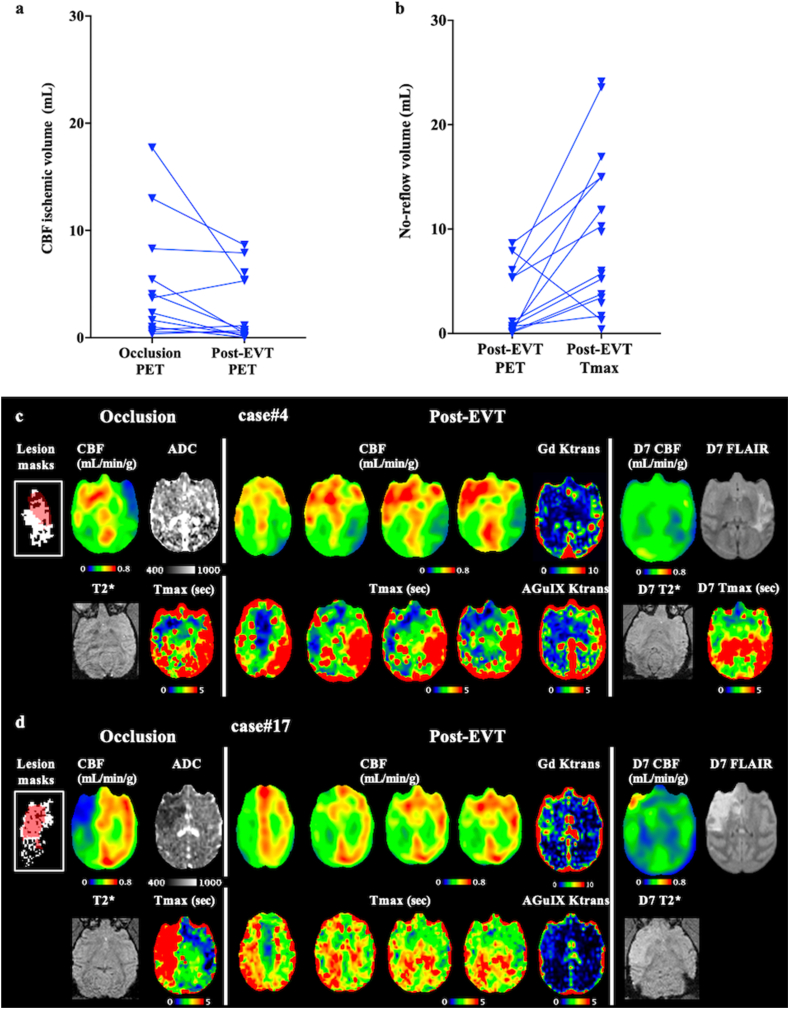
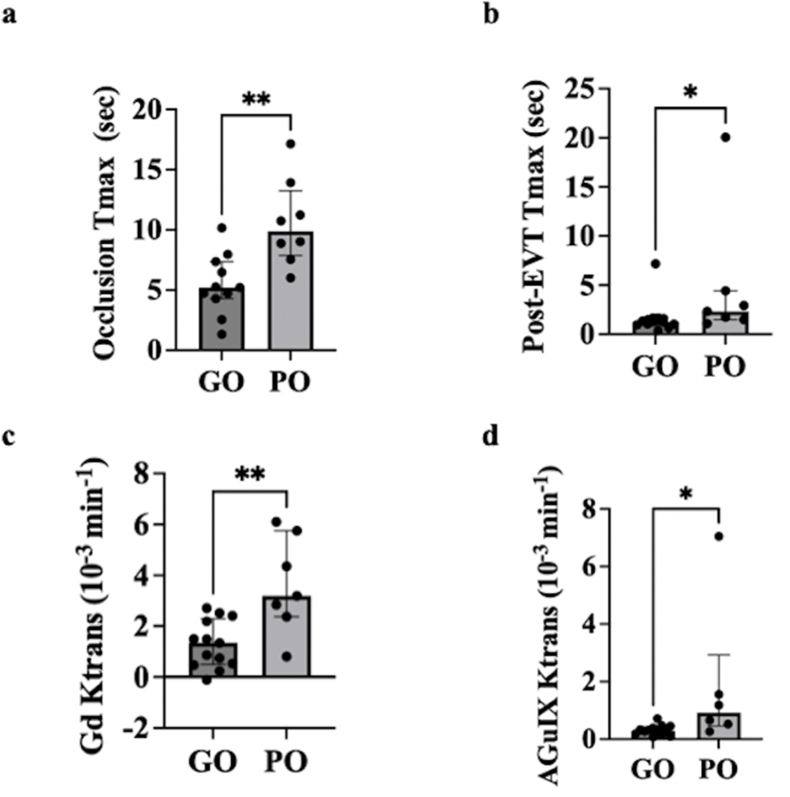
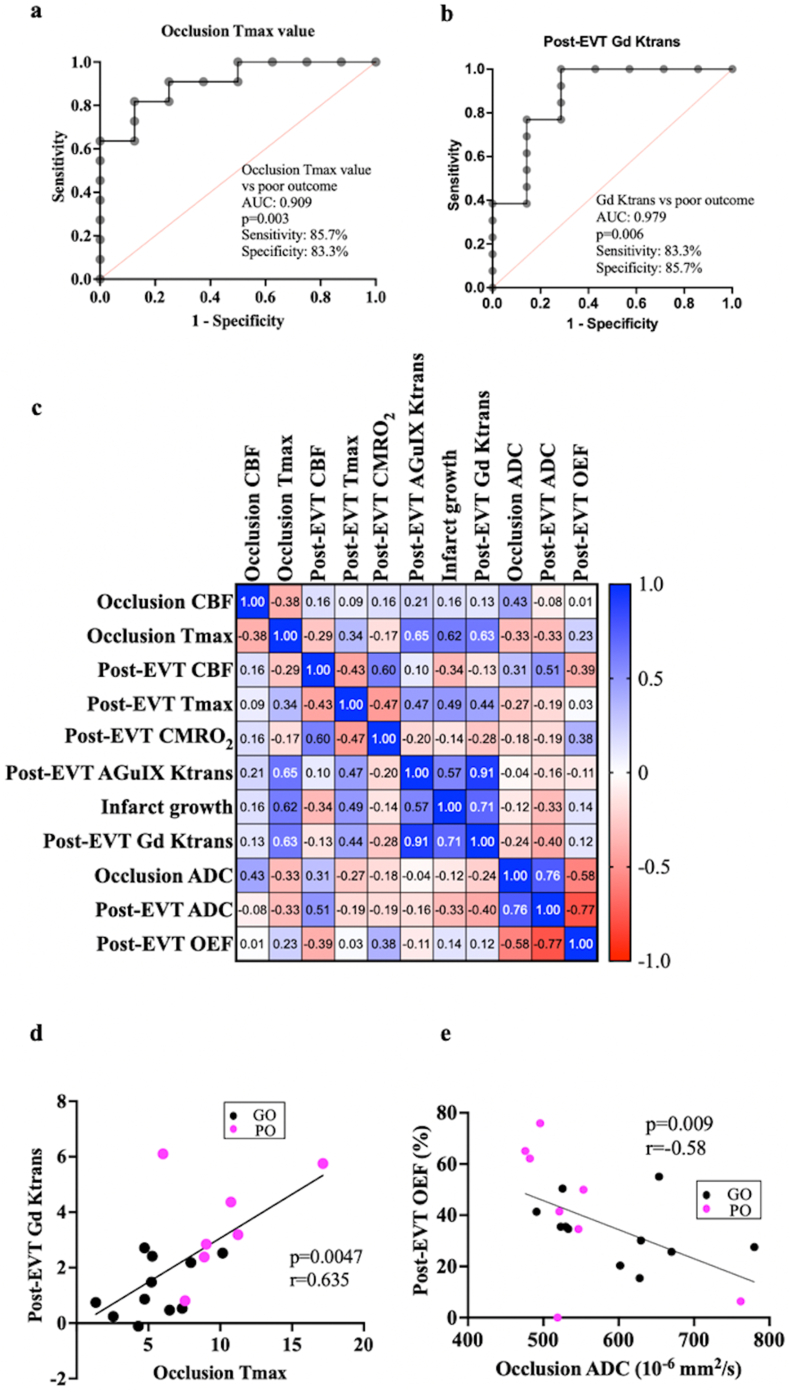
Microvascular dysfunction and no-reflow are considered a major cause of secondary damage despite revascularization in acute ischemic stroke (AIS), ultimately affecting patient outcomes. We used quantitative PET-MRI imaging to characterize early microvascular damages in a preclinical non-human primate model mimicking endovascular mechanical thrombectomy (EVT). During occlusion, PET perfusion and MRI diffusion were used to measure ischemic and lesion core volumes respectively. Following revascularization, multiparametric PET-MRI included perfusion, diffusion, blood-brain barrier (BBB) permeability MRI, and O-oxygen metabolism PET. Lesion growth on MRI was evaluated at one week, and the neurological score was assessed daily; a poor outcome was defined as a score>6 (0-normal, 60-death) after one week. Early after recanalization, the gold-standard PET ischemic threshold (<0.2 mL/min/g) identified post-EVT hypoperfusion in 67 % of the cases (14/21) located in the occlusion acute lesion. Acquired 110 min post-EVT, the area of MRI Tmax hypoperfusion was larger and even more frequent (18/20) and was also located within the acute lesion. Eight of the total cases (38 %) had a poor outcome, and all of them had no-reflow (7/8 MRI no-reflow and 6/8 PET no-reflow). Diffusion ADC alterations and post-EVT oxygen extraction fraction (OEF) values were significantly different in PET no-reflow cases compared to those without no-reflow, exhibiting an inverse correlation. Independently of no-reflow, long perfusion Tmax and post-EVT high BBB Ktrans in the lesion core were the hallmarks of poor outcome and infarct growth. This early quantitative imaging signature may predict infarct growth and poor outcome and help to identify neuroprotection targets.
微血管功能障碍和无复流现象被认为是急性缺血性卒中(AIS)血管再通后继发性损伤的主要原因,最终影响患者预后。我们使用定量PET-MRI成像技术,在模拟血管内机械取栓术(EVT)的临床前非人类灵长类动物模型中,对早期微血管损伤进行特征描述。在闭塞期间,PET灌注和MRI扩散分别用于测量缺血体积和梗死核心体积。血管再通后,多参数PET-MRI包括灌注、扩散、血脑屏障(BBB)通透性MRI和氧代谢PET。在一周时评估MRI上的病灶生长情况,并每日评估神经学评分;不良预后定义为一周后评分>6(0-正常,60-死亡)。再通后早期,金标准PET缺血阈值(<0.2 mL/min/g)在67%(14/21)位于闭塞急性病灶处的病例中识别出EVT后灌注不足。在EVT后110分钟获得的数据显示,MRI Tmax灌注不足区域更大且更常见(18/20),且也位于急性病灶内。总病例中有8例(38%)预后不良,且所有这些病例均存在无复流现象(7/8 MRI无复流和6/8 PET无复流)。与无无复流现象的病例相比,PET无复流病例中的扩散ADC改变和EVT后氧摄取分数(OEF)值存在显著差异,呈负相关。独立于无复流现象之外,病灶核心区域灌注Tmax时间长和EVT后BBB Ktrans值高是预后不良和梗死灶生长的标志。这种早期定量成像特征可能预测梗死灶生长和不良预后,并有助于识别神经保护靶点。