Rhee June-Wha, Pillai Raju, Chen Sitong, Bosworth Alysia, Oganesyan Artem, Atencio Liezl, Freeman Kendall, Estrada Caitlyn, Guzman Tati, Lukas Kara, Peng Kelly, Sigala Brianna, Lukuridze Aleksi, Lindenfeld Lanie, Jamal Faizi, Natarajan Pradeep, Bhatia Smita, Herrera Alex F, Mei Matthew G, Nakamura Ryotaro, Wong F Lennie, Forman Stephen J, Armenian Saro H
Department of Medicine, City of Hope Comprehensive Cancer Center, Duarte, California, USA.
Department of Pathology, City of Hope Comprehensive Cancer Center, Duarte, California, USA.
JACC CardioOncol. 2024 Dec 3;7(1):20-33. doi: 10.1016/j.jaccao.2024.10.006. eCollection 2025 Jan.
Patients with lymphoma are at high risk for developing heart failure (HF) after autologous hematopoietic cell transplantation (HCT). More accurate risk determination pre-HCT may facilitate screening and prevention of HF.
The aim of this study was to examine the association between clonal hematopoiesis of indeterminate potential (CHIP) and the risk for HF after HCT for lymphoma.
This was a retrospective cohort study of 861 patients who underwent autologous HCT for lymphoma between 2010 and 2016 at City of Hope Comprehensive Cancer Center. Targeted DNA sequencing was performed to determine the presence of CHIP (variant allele frequency ≥ 2%). The primary outcome of interest was the 5-year cumulative incidence of de novo HF. Other outcomes of interest included overall and cause-specific mortality.
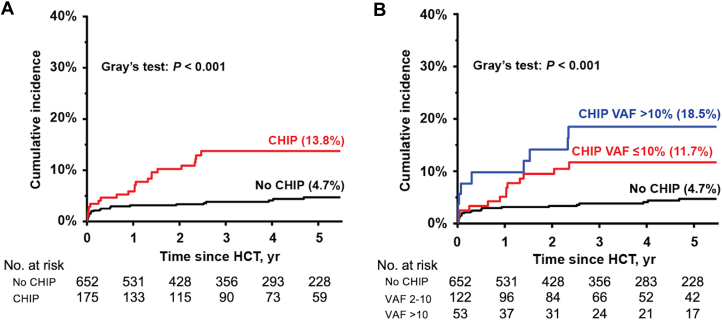
Overall, 186 patients (21.7% of the cohort) had at least 1 CHIP variant, and 59 (6.9%) had ≥2 variants. , , and were the most frequently mutated genes. The 5-year incidence of HF was significantly higher in patients with CHIP compared with those without CHIP (13.8% vs 4.7%; < 0.001; sub-distribution hazard ratio [sHR]: 2.48; 95% CI: 1.32-4.68); the HF incidence increased by variant allele frequency: 0-2% (4.7%), 2-10% (11.7%), and >10% (18.5%), < 0.001. Patients with CHIP had significantly worse overall survival after HCT, compared with those without (63.4% vs 80.3%; < 0.001), due primarily to the higher risk for nonrelapse mortality (subdistribution HR: 5.37; 95% CI: 2.34-12.35).
CHIP was highly prevalent and associated with risk for HF and nonrelapse mortality after HCT. These findings highlight the role of CHIP as a novel biomarker and potential target for intervention to improve outcomes after autologous HCT.
淋巴瘤患者在自体造血细胞移植(HCT)后发生心力衰竭(HF)的风险很高。HCT前更准确的风险判定可能有助于HF的筛查和预防。
本研究旨在探讨不确定潜能克隆造血(CHIP)与淋巴瘤HCT后HF风险之间的关联。
这是一项对2010年至2016年间在希望之城综合癌症中心接受淋巴瘤自体HCT的861例患者进行的回顾性队列研究。进行靶向DNA测序以确定CHIP(变异等位基因频率≥2%)的存在情况。主要关注的结局是新发HF的5年累积发生率。其他关注的结局包括总死亡率和特定病因死亡率。
总体而言,186例患者(占队列的21.7%)至少有1个CHIP变异,59例(6.9%)有≥2个变异。 、 和 是最常发生突变的基因。与无CHIP的患者相比,有CHIP的患者HF的5年发生率显著更高(13.8%对4.7%; <0.001;亚分布风险比[sHR]:2.48;95%CI:1.32 - 4.68);HF发生率随变异等位基因频率增加:0 - 2%(4.7%)、2 - 10%(11.7%)和>10%(18.5%), <0.001。与无CHIP的患者相比,有CHIP的患者HCT后的总生存期显著更差(63.4%对80.3%; <0.001),主要原因是非复发死亡率更高(亚分布HR:5.37;95%CI:2.34 - 12.35)。
CHIP在HCT后非常普遍,且与HF风险和非复发死亡率相关。这些发现凸显了CHIP作为一种新型生物标志物的作用以及作为改善自体HCT后结局的潜在干预靶点的作用。