School of Public Health, The University of Texas Health Science Center at Houston, Houston, Texas, USA.
Center for Primary Care and Prevention, Brown University, Pawtucket, Rhode Island, USA.
J Am Coll Cardiol. 2021 Jul 6;78(1):42-52. doi: 10.1016/j.jacc.2021.04.085.
Age-related clonal hematopoiesis of indeterminate potential (CHIP), defined as clonally expanded leukemogenic sequence variations (particularly in DNMT3A, TET2, ASXL1, and JAK2) in asymptomatic individuals, is associated with cardiovascular events, including recurrent heart failure (HF).
This study sought to evaluate whether CHIP is associated with incident HF.
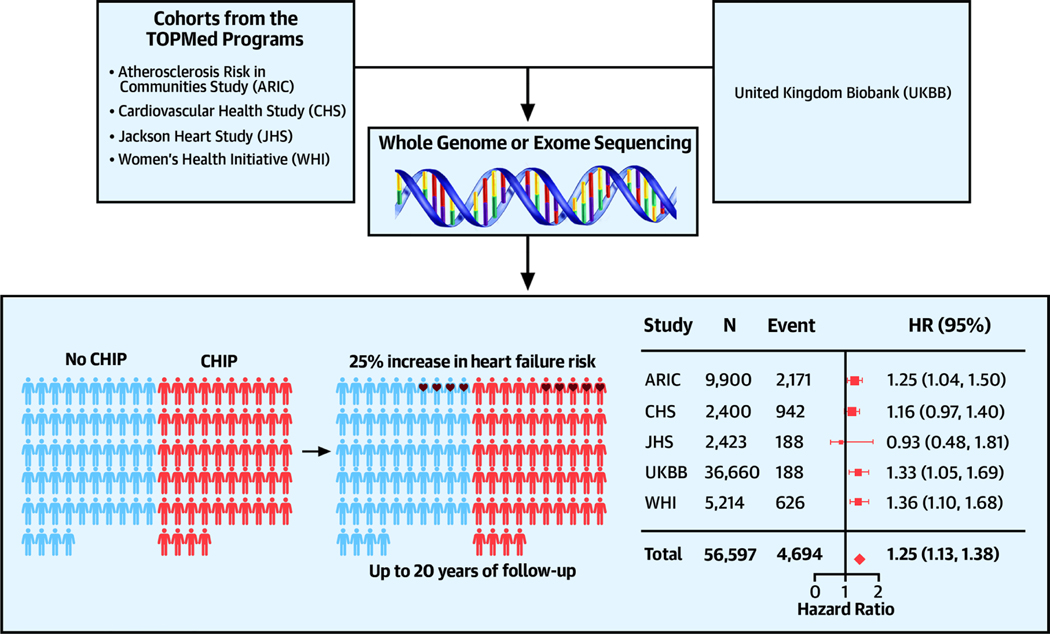
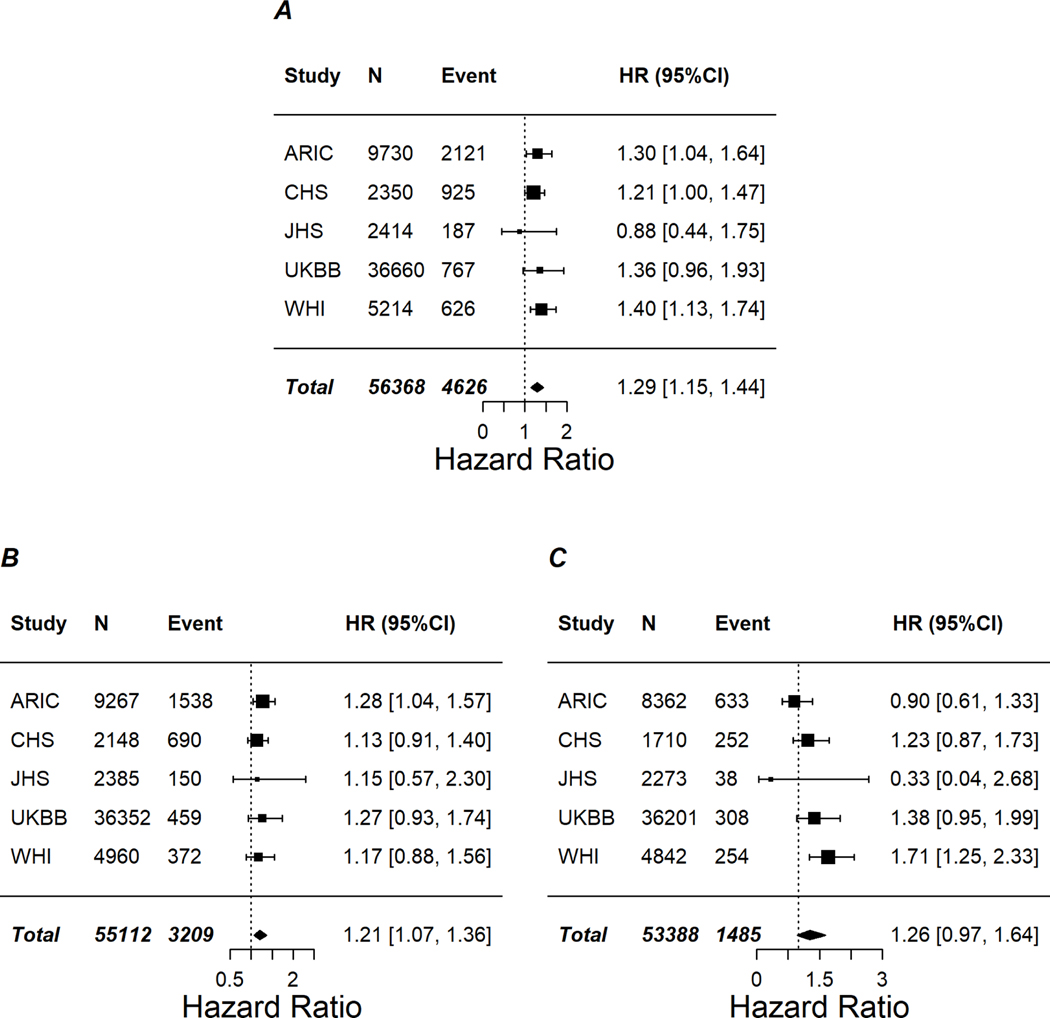
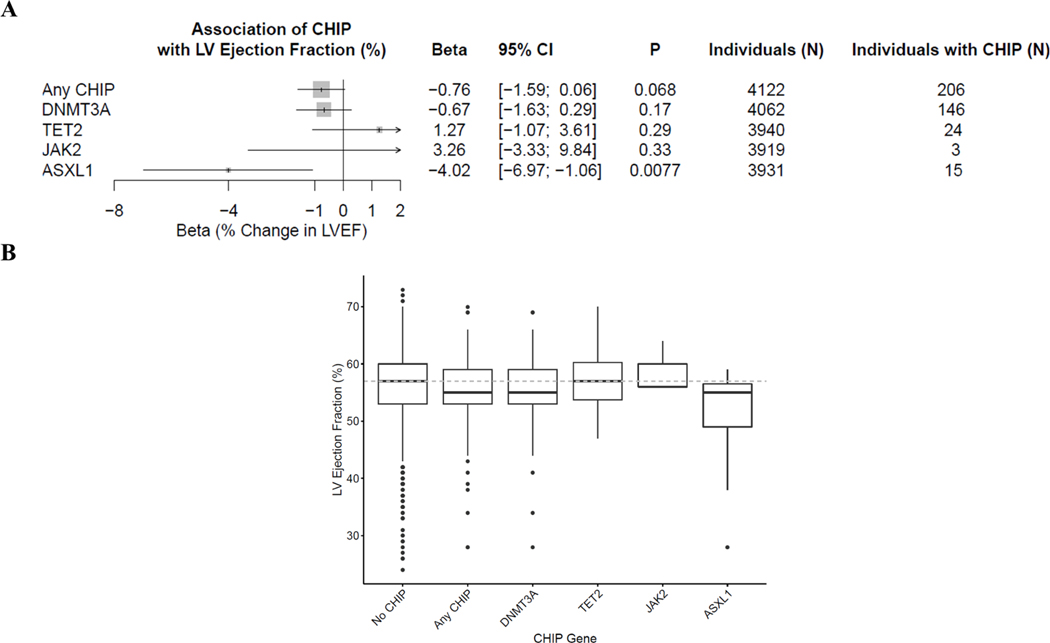
CHIP status was obtained from whole exome or genome sequencing of blood DNA in participants without prevalent HF or hematological malignancy from 5 cohorts. Cox proportional hazards models were performed within each cohort, adjusting for demographic and clinical risk factors, followed by fixed-effect meta-analyses. Large CHIP clones (defined as variant allele frequency >10%), HF with or without baseline coronary heart disease, and left ventricular ejection fraction were evaluated in secondary analyses.
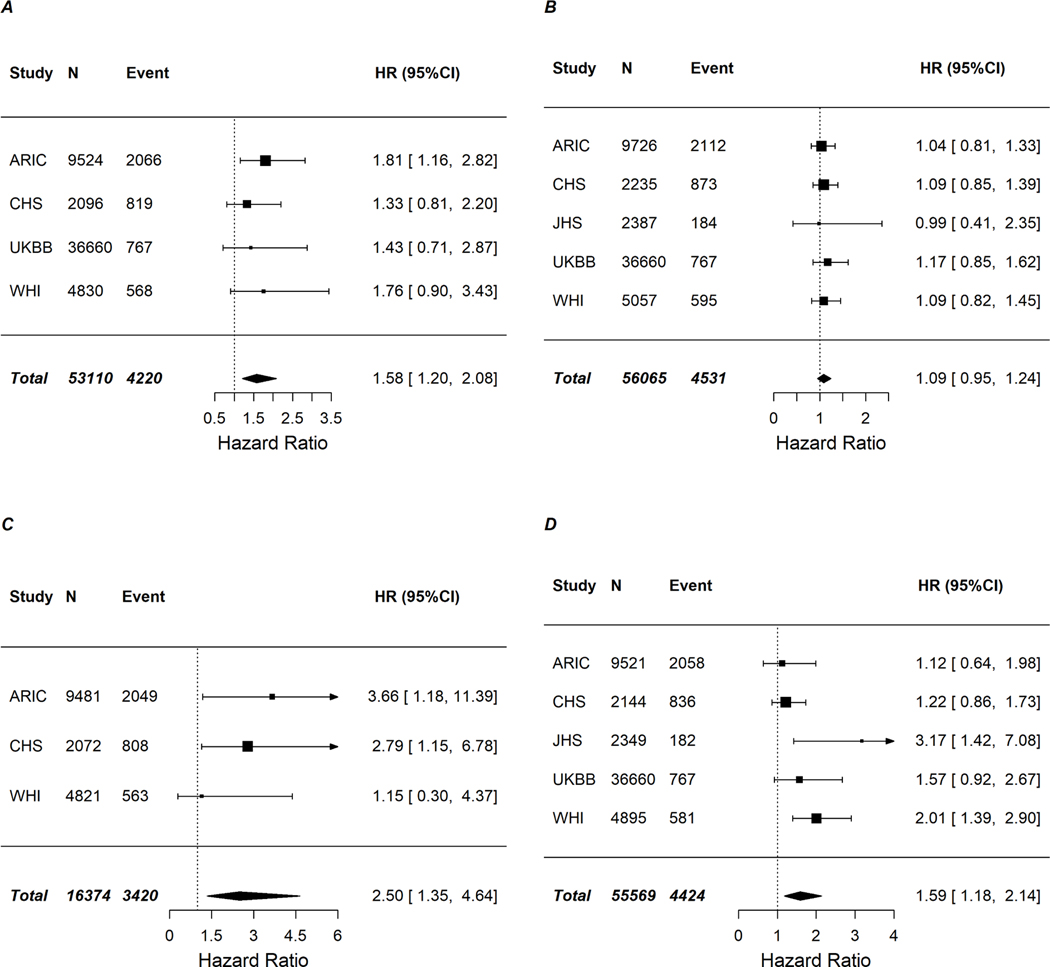
Of 56,597 individuals (59% women, mean age 58 years at baseline), 3,406 (6%) had CHIP, and 4,694 developed HF (8.3%) over up to 20 years of follow-up. CHIP was prospectively associated with a 25% increased risk of HF in meta-analysis (hazard ratio: 1.25; 95% confidence interval: 1.13-1.38) with consistent associations across cohorts. ASXL1, TET2, and JAK2 sequence variations were each associated with an increased risk of HF, whereas DNMT3A sequence variations were not associated with HF. Secondary analyses suggested large CHIP was associated with a greater risk of HF (hazard ratio: 1.29; 95% confidence interval: 1.15-1.44), and the associations for CHIP on HF with and without prior coronary heart disease were homogenous. ASXL1 sequence variations were associated with reduced left ventricular ejection fraction.
CHIP, particularly sequence variations in ASXL1, TET2, and JAK2, represents a new risk factor for HF.
与心血管事件相关的年龄相关不确定潜能克隆性造血(CHIP),定义为无症状个体中克隆性扩展的白血病序列变异(特别是在 DNMT3A、TET2、ASXL1 和 JAK2 中),包括复发性心力衰竭(HF)。
本研究旨在评估 CHIP 是否与 HF 事件相关。
从 5 个队列中无明显 HF 或血液恶性肿瘤的参与者的血液 DNA 进行全外显子或全基因组测序,以获得 CHIP 状态。在每个队列中进行 Cox 比例风险模型分析,调整人口统计学和临床危险因素,然后进行固定效应荟萃分析。在次级分析中评估了较大的 CHIP 克隆(定义为变异等位基因频率>10%)、伴有或不伴有基线冠心病的 HF 和左心室射血分数。
在 56597 名参与者(59%为女性,基线时平均年龄为 58 岁)中,3406 名(6%)存在 CHIP,4694 名在长达 20 年的随访中发生 HF(8.3%)。荟萃分析显示,CHIP 与 HF 风险增加 25%相关(风险比:1.25;95%置信区间:1.13-1.38),且各队列的相关性一致。ASXL1、TET2 和 JAK2 序列变异均与 HF 风险增加相关,而 DNMT3A 序列变异与 HF 无关。次级分析表明,较大的 CHIP 与 HF 风险增加相关(风险比:1.29;95%置信区间:1.15-1.44),且 CHIP 与无先前冠心病 HF 之间的关联具有同质性。ASXL1 序列变异与左心室射血分数降低相关。
CHIP,特别是 ASXL1、TET2 和 JAK2 的序列变异,代表 HF 的一个新的危险因素。