Westin Jason, Phillips Tycel J, Mehta Amitkumar, Hoffmann Marc S, Gonzalez-Barca Eva, Thieblemont Catherine, Bastos-Oreiro Mariana, Greil Richard, Giebel Sebastian, Wei Michael C, Wang Jue, Bucher Reinhard, Sit Jason, Penuel Elicia, Purev Enkhtsetseg, Yee Donald L, Bergua-Burgues Juan Miguel
Department of Lymphoma & Myeloma, The University of Texas MD Anderson Cancer Center, Houston, TX.
Department of Internal Medicine, Division of Hematology and Oncology, University of Michigan, Ann Arbor, MI.
Blood Adv. 2025 May 27;9(10):2461-2472. doi: 10.1182/bloodadvances.2024014907.
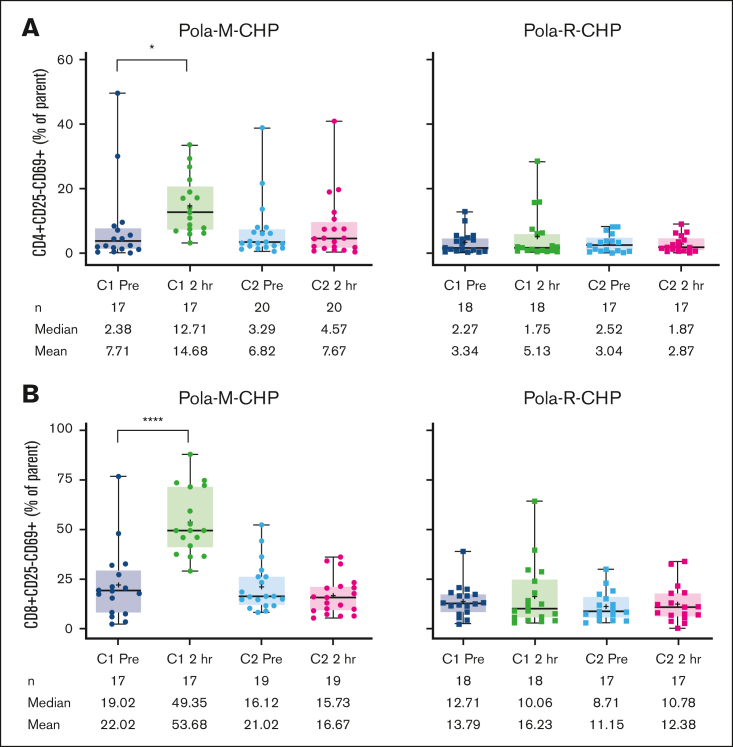
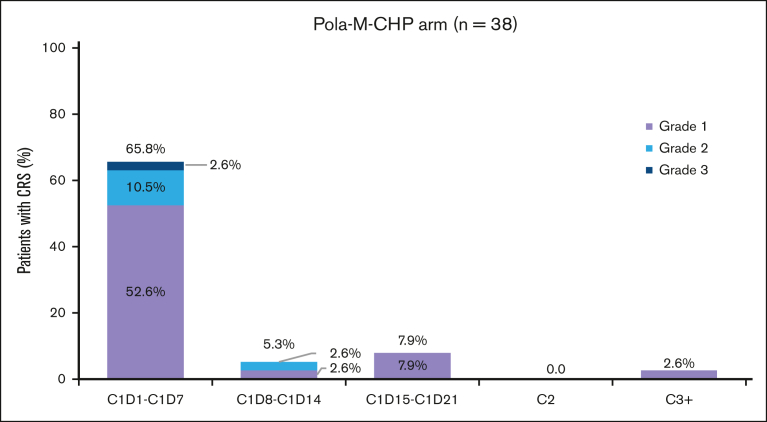
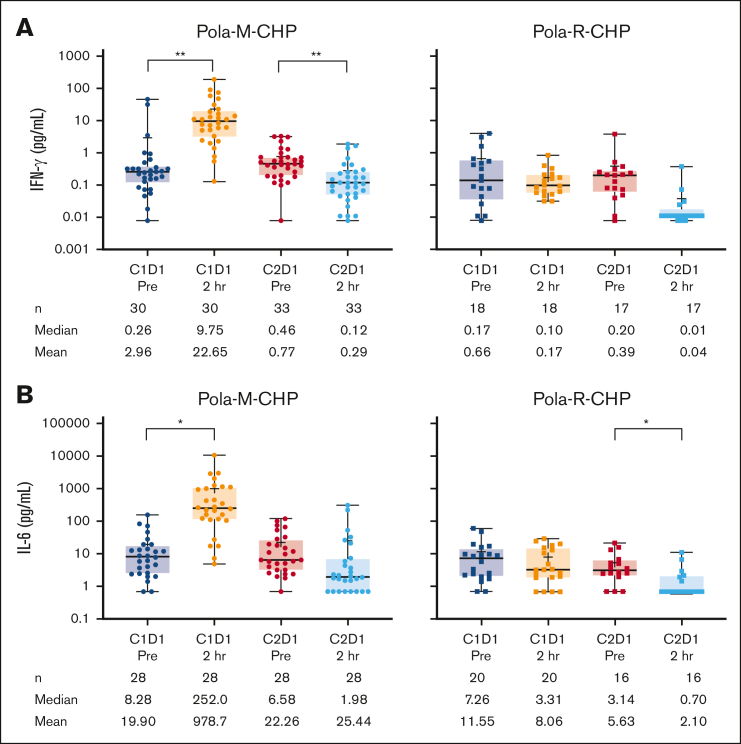
This phase 2 study evaluated mosunetuzumab plus cyclophosphamide, doxorubicin, prednisone, and polatuzumab vedotin (Pola-M-CHP) vs Pola-rituximab (R)-CHP for first-line treatment of diffuse large B-cell lymphoma. Patients were randomized 2:1 to receive 6 cycles of Pola-M-CHP or Pola-R-CHP on day 1 of each 21-day cycle. Mosunetuzumab was administered intravenously via step-up dosing during cycle 1 and at 30 mg on day 1 of subsequent cycles. The primary end point was independent review committee-assessed complete response (CR) rate by positron emission tomography-computed tomography. Overall, 62 patients were enrolled and received Pola-M-CHP (n = 40) or Pola-R-CHP (n = 22). CR rates were similar in both arms (72.5% with Pola-M-CHP vs 77.3% with Pola-R-CHP); the 24-month investigator-assessed progression-free survival rate was 70.8% (95% confidence interval [CI], 55.6-86.1) with Pola-M-CHP vs 81.8% (95% CI, 65.7-97.9) with Pola-R-CHP. The most common adverse event (AE) was cytokine release syndrome (68.4%; mostly grade 1 [52.6%], and primarily confined to cycle 1) with Pola-M-CHP and neutropenia/neutrophil count decreased (54.5%) with Pola-R-CHP. Neutropenia/neutrophil count decreased was the most frequently observed grade ≥3 AE in both arms (Pola-M-CHP, 36.8%; Pola-R-CHP, 22.7%). Rates of grade ≥3 AEs (86.8% vs 59.1%), serious AEs (63.2% vs 13.6%), and AEs leading to treatment discontinuation (13.2% vs 0%) were higher with Pola-M-CHP than Pola-R-CHP, respectively. Pharmacodynamic changes were supportive of mosunetuzumab's mechanism of action and its addition to the Pola-CHP combination. Pola-M-CHP, although an active combination, did not demonstrate a clinical benefit over Pola-R-CHP in this small study. This trial was registered at www.clinicaltrials.gov as #NCT03677141.
这项2期研究评估了mosunetuzumab联合环磷酰胺、多柔比星、泼尼松和泊洛妥珠单抗(Pola-M-CHP)与Pola-利妥昔单抗(R)-CHP用于一线治疗弥漫性大B细胞淋巴瘤的疗效。患者按2:1随机分组,在每21天周期的第1天接受6个周期的Pola-M-CHP或Pola-R-CHP治疗。Mosunetuzumab在第1周期通过逐步递增剂量静脉给药,后续周期第1天给予30mg。主要终点是独立审查委员会通过正电子发射断层扫描-计算机断层扫描评估的完全缓解(CR)率。总体而言,62例患者入组并接受了Pola-M-CHP(n = 40)或Pola-R-CHP(n = 22)治疗。两组的CR率相似(Pola-M-CHP为72.5%,Pola-R-CHP为77.3%);Pola-M-CHP组24个月时研究者评估的无进展生存率为70.8%(95%置信区间[CI],55.6 - 86.1),Pola-R-CHP组为81.8%(95%CI,65.7 - 97.9)。最常见的不良事件(AE)是Pola-M-CHP组的细胞因子释放综合征(68.4%;大多为1级[52.6%],主要局限于第1周期)和Pola-R-CHP组的中性粒细胞减少/中性粒细胞计数降低(54.5%)。中性粒细胞减少/中性粒细胞计数降低是两组中最常观察到的≥3级AE(Pola-M-CHP组为36.8%;Pola-R-CHP组为22.7%)。Pola-M-CHP组≥3级AE发生率(86.8%对59.1%)、严重AE发生率(63.2%对13.6%)和导致治疗中断的AE发生率(13.2%对0%)均高于Pola-R-CHP组。药效学变化支持mosunetuzumab的作用机制及其加入Pola-CHP联合方案。在这项小型研究中,Pola-M-CHP虽然是一种有效的联合方案,但未显示出比Pola-R-CHP有临床益处。该试验在www.clinicaltrials.gov上注册,编号为#NCT03677141。