Lifespan Cancer Institute, Warren Alpert Medical School of Brown University, Providence, RI.
Division of Hematology and Oncology, University of Michigan, Ann Arbor, MI.
Blood Adv. 2023 Oct 24;7(20):6055-6065. doi: 10.1182/bloodadvances.2023010840.
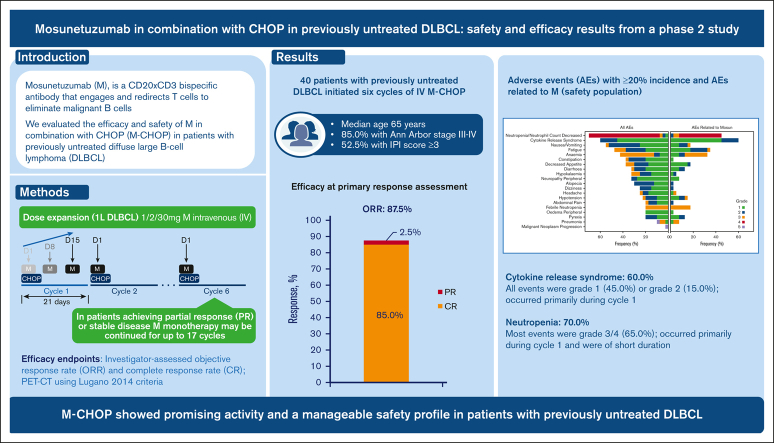
Up to 40% of patients with diffuse large B-cell lymphoma (DLBCL) are refractory to or relapse after first-line therapy, highlighting the need for better treatments. Mosunetuzumab is a CD20 × CD3 bispecific antibody that engages and redirects T cells to eliminate malignant B cells. In this phase 2, open-label study (NCT03677141), 40 patients (52.5% with international prognostic index ≥3) with previously untreated DLBCL initiated 6 cycles of IV mosunetuzumab with CHOP (cyclophosphamide, doxorubicin, vincristine, and prednisone) chemotherapy. Mosunetuzumab was administered in cycle 1 as step-up doses to mitigate cytokine release syndrome [CRS], and a dose of 30 mg was given on day 1 of cycles 2-6. Efficacy end points included objective and complete response rates, as determined by the investigator, via positron emission tomography-computed tomography, using Lugano 2014 criteria (87.5% and 85.0%, respectively). At a median follow-up of 32.0 months, the estimated 2-year progression-free survival and event-free survival rates were 65.4% (95% confidence interval [CI], 49.5-81.4) and 60.4% (95% CI, 44.7-76.1), respectively. CRS occurred in 60.0% of patients; all events were grade 1 (45.0%) or grade 2 (15.0%) and occurred primarily in cycle 1. Mosunetuzumab-related grade ≥3 neurologic adverse events (AEs) potentially consistent with immune effector cell-associated neurotoxicity syndrome occurred in 1 patient (2.5%). Grade 5 AEs were reported in 2 patients. Neutropenia occurred in 70.0% of patients, mostly during cycle 1 and was of short duration. These findings demonstrate promising activity and a manageable safety profile for mosunetuzumab-CHOP and warrant further investigation of mosunetuzumab in first-line combination regimens for DLBCL.
多达 40%的弥漫性大 B 细胞淋巴瘤 (DLBCL) 患者对一线治疗无反应或复发,这突显了需要更好的治疗方法。Mosunetuzumab 是一种 CD20×CD3 双特异性抗体,可招募和重定向 T 细胞以消除恶性 B 细胞。在这项 2 期、开放标签研究(NCT03677141)中,40 名未经治疗的 DLBCL 患者(52.5%的患者国际预后指数≥3)接受了 6 个周期的 IV mosunetuzumab 联合 CHOP(环磷酰胺、多柔比星、长春新碱和泼尼松)化疗。在第 1 周期中,mosunetuzumab 以递增剂量给药以减轻细胞因子释放综合征 [CRS],并在第 2-6 周期的第 1 天给予 30mg 剂量。疗效终点包括通过正电子发射断层扫描-计算机断层扫描(使用 Lugano 2014 标准)由研究者确定的客观缓解率和完全缓解率(分别为 87.5%和 85.0%)。在中位随访 32.0 个月时,估计 2 年无进展生存率和无事件生存率分别为 65.4%(95%置信区间[CI],49.5-81.4)和 60.4%(95%CI,44.7-76.1)。60.0%的患者发生 CRS;所有事件均为 1 级(45.0%)或 2 级(15.0%),主要发生在第 1 周期。1 名患者(2.5%)发生与免疫效应细胞相关的神经毒性综合征(immune effector cell-associated neurotoxicity syndrome,ICANS)一致的 mosunetuzumab 相关≥3 级神经系统不良事件(AE)。2 名患者发生 5 级 AE。70.0%的患者发生中性粒细胞减少症,主要发生在第 1 周期,持续时间较短。这些发现表明 mosunetuzumab-CHOP 具有有前景的活性和可管理的安全性特征,值得进一步研究 mosunetuzumab 在 DLBCL 的一线联合治疗方案中的应用。