VandeVrede Lawren, Cho Hanna, Sanderson-Cimino Mark, Wekselman Fattin, Cobigo Yann, Gorno-Tempini Maria Luisa, Heuer Hilary W, Kramer Joel H, Lario Lago Argentina, Leichter Dana, Ljubenkov Peter, Miller Bruce L, Perry David C, Rabinovici Gil D, Rojas Julio C, Rosen Howard J, Saloner Rowan, Staffaroni Adam, Triana-Baltzer Gallen, Spina Salvatore, Seeley William W, Grinberg Lea T, Kolb Hartmuth C, La Joie Renaud, Boxer Adam L
Memory and Aging Center, UCSF Weill Institute for Neurosciences, University of California, San Francisco.
Department of Neurology, Gangnam Severance Hospital, Yonsei University College of Medicine, Seoul, Republic of Korea.
JAMA Neurol. 2025 Feb 10;82(4):344-54. doi: 10.1001/jamaneurol.2024.5017.
Blood-based biomarkers for Alzheimer disease (AD) are clinically available, but their value is not well understood in syndromes typically associated with frontotemporal lobar degeneration syndromes (FTLD).
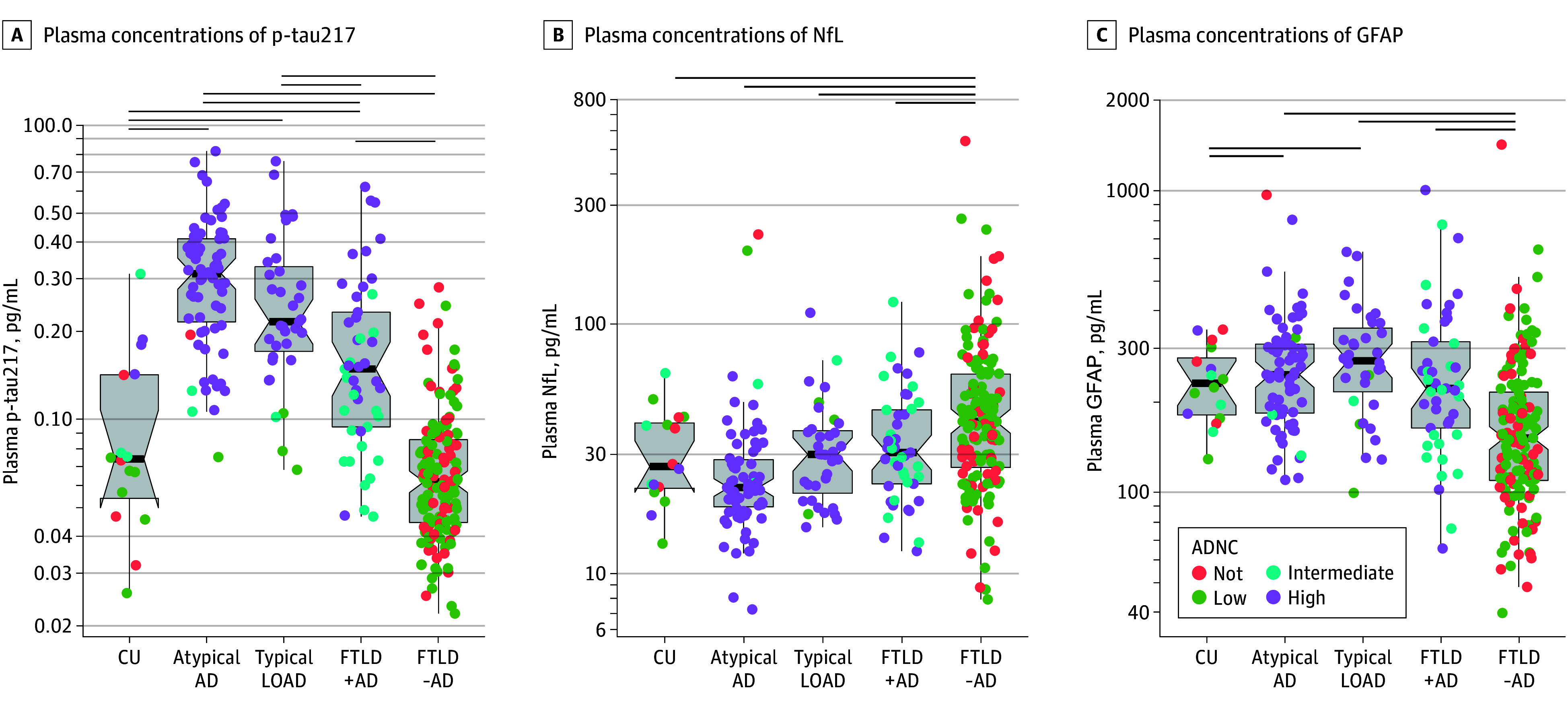
To investigate the clinical importance and detectability of AD in FTLD-related neurodegenerative syndromes using 3 plasma biomarkers, phosphorylated tau 217 (p-tau217), neurofilament light chain (NfL), and glial fibrillary acidic protein (GFAP).
DESIGN, SETTING, AND PARTICIPANTS: This clinicopathological study took place at the University of California San Francisco Alzheimer Disease Research Center from August 2008 to July 2022. Autopsied individuals with clinical evaluation and neuropathological examination, diagnosed with clinical syndromes related to AD (n = 125), frontotemporal lobar degeneration (FTLD; n = 198), or cognitively unimpaired (CU) at the time of evaluation (n = 16) were included.
AD-related or FTLD-related clinical syndromes or CU.
P-tau217, NfL, and GFAP were measured with single-molecule array (SIMOA). AD was defined as intermediate or high AD neuropathological change (ADNC) at autopsy. Clinical biomarker associations were evaluated using linear regressions. Imaging analyses used bayesian linear mixed-effects modeling.
A total of 349 individuals (191 [55%] male; mean [SD] age at death, 72 [11] years) were included. AD was common in both AD-related syndromes (110/125 [88%]) and FTLD-related syndromes (45/198 [23%]). Neuropathological stage at autopsy was higher in AD-related syndromes (high ADNC: 82/88 [93%] AD vs 13/23 [56%] FTLD), and AD was frequently considered a copathology in FTLD-related syndromes (30/198 [15%]). Plasma p-tau217 concentrations were higher in AD-related syndromes (mean [SD], 0.28 [0.16] pg/mL) than FTLD-related syndromes (mean [SD], 0.10 [0.09] pg/mL) (P < .05). Plasma p-tau217 concentrations were highest in atypical AD-related syndromes (mean [SD], 0.33 [0.02] pg/mL), followed by typical late-onset amnestic syndromes (mean [SD], 0.27 [0.03] pg/mL). FTLD-related syndromes with AD (mean [SD], 0.19 [0.02] pg/mL) were higher compared to without (mean [SD], 0.07 [0.00] pg/mL). Plasma p-tau217 detected AD neuropathology across syndromes (area under the receiver operating characteristic curve [AUC], 0.95; 95% CI, 0.93-0.97), with slightly better performance in AD-related syndromes (AUC, 0.98; 95% CI, 0.95-1.00) compared to FTLD-related syndromes (AUC, 0.89; 95% CI, 0.83-0.94). NfL and GFAP had lower performance for detecting AD (AUC, 0.73; 95% CI, 0.68-0.78 and AUC, 0.75; 95% CI, 0.67-0.80, respectively) and added little to no diagnostic value either alone or in combinations with p-tau217. The presence of AD in FTLD-related syndromes was associated with lower Mini-Mental State Examination score (mean [SD], -2.90 [1.09]; P < .05), worse performance on memory (mean [SD] z score, -0.64 [0.32]), executive (mean [SD] z score, -0.74 [0.19]), and visuospatial composites (mean [SD] z score, -0.88 [0.37]) as well as increased rates of posterior cortical atrophy.
Clinically relevant AD was prevalent across neurodegenerative syndromes and detectable with plasma p-tau217. Plasma p-tau217 may be a useful tool to investigate the clinical impact of AD copathology in non-AD neurodegenerative syndromes, including the effect of disease-modifying therapies.
用于阿尔茨海默病(AD)的血液生物标志物已可用于临床,但在通常与额颞叶变性综合征(FTLD)相关的综合征中,其价值尚未得到充分理解。
使用三种血浆生物标志物,即磷酸化tau 217(p-tau217)、神经丝轻链(NfL)和胶质纤维酸性蛋白(GFAP),研究FTLD相关神经退行性综合征中AD的临床重要性和可检测性。
设计、设置和参与者:这项临床病理研究于2008年8月至2022年7月在加利福尼亚大学旧金山分校阿尔茨海默病研究中心进行。纳入了经过临床评估和神经病理学检查的尸检个体,他们在评估时被诊断为与AD相关的临床综合征(n = 125)、额颞叶变性(FTLD;n = 198)或认知未受损(CU)(n = 16)。
与AD相关或与FTLD相关的临床综合征或CU。
使用单分子阵列(SIMOA)测量p-tau217、NfL和GFAP。AD在尸检时被定义为中度或高度AD神经病理改变(ADNC)。使用线性回归评估临床生物标志物关联。成像分析采用贝叶斯线性混合效应模型。
共纳入349名个体(191名[55%]男性;死亡时的平均[标准差]年龄为72[11]岁)。AD在与AD相关的综合征(110/125[88%])和与FTLD相关的综合征(45/198[23%])中都很常见。与AD相关的综合征在尸检时的神经病理分期更高(高度ADNC:82/88[93%]AD vs 13/23[56%]FTLD),并且AD在与FTLD相关的综合征中经常被视为合并病理(30/198[15%])。与FTLD相关的综合征相比,与AD相关的综合征的血浆p-tau217浓度更高(平均[标准差],0.28[0.16]pg/mL对0.10[0.09]pg/mL)(P <.05)。血浆p-tau217浓度在非典型AD相关综合征中最高(平均[标准差],0.33[0.02]pg/mL),其次是典型的晚发性遗忘综合征(平均[标准差],0.27[0.03]pg/mL)。与无AD的FTLD相关综合征(平均[标准差],0.07[0.00]pg/mL)相比,伴有AD的FTLD相关综合征(平均[标准差])为0.19[0.02]pg/mL)更高。血浆p-tau217在各种综合征中均能检测到AD神经病理(受试者操作特征曲线下面积[AUC],0.95;95%CI,0.93 - 0.97),与FTLD相关综合征(AUC,0.89;95%CI,0.83 - 0.94)相比,在与AD相关的综合征中的表现略好(AUC,0.98;95%CI,0.95 - 1.00)。NfL和GFAP在检测AD方面表现较差(AUC分别为0.73;95%CI,0.68 - 0.78和AUC,0.75;95%CI,0.67 - 0.80),单独或与p-tau217联合使用时几乎没有增加诊断价值。与FTLD相关综合征中AD的存在与较低的简易精神状态检查得分(平均[标准差],-2.90[1.09];P <.