Kahle Ann-Kathrin, Alken Fares-Alexander, Scherschel Katharina, Zhu Ernan, Gunawardene Melanie A, Metzner Andreas, Willems Stephan, Meyer Christian
Division of Cardiology, Angiology, Intensive Care Medicine, EVK Düsseldorf, cNEP, cardiac Neuro- and Electrophysiology Research Consortium, Kirchfeldstrasse 40, 40217 Düsseldorf, Germany.
Department of Cardiology, Pulmonology and Vascular Medicine, Medical Faculty, University Hospital Düsseldorf, Moorenstrasse 5, 40225 Düsseldorf, Germany.
J Clin Med. 2025 Jan 21;14(3):675. doi: 10.3390/jcm14030675.
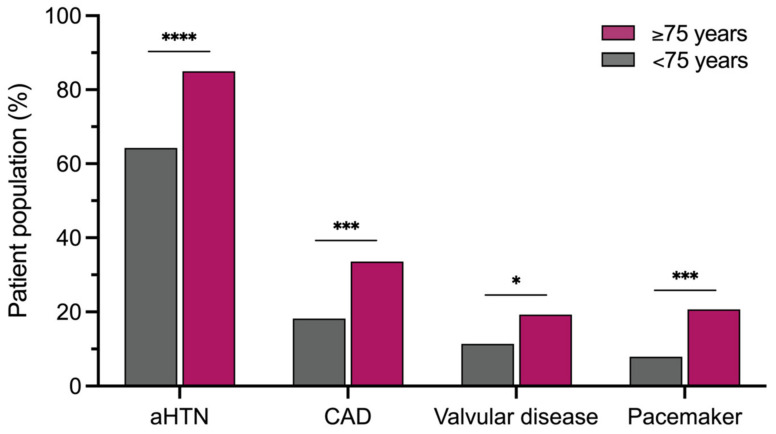
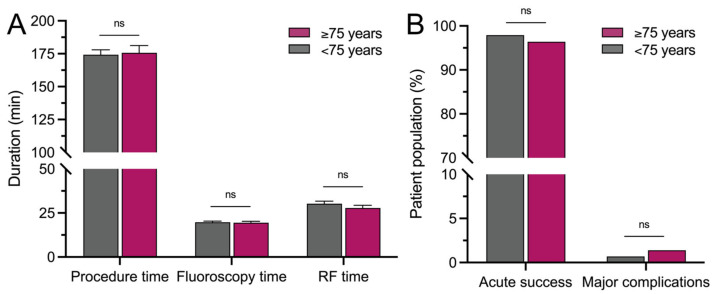
Age is a relevant risk factor for the development of atrial arrhythmias and an independent predictor of adverse cardiovascular outcomes. The incidence of atrial tachycardia (AT) is known to increase with aging, but so far, there are no data on elderly patients with AT. Therefore, we sought to assess the safety and outcomes of AT ablation in patients ≥75 years compared to those <75 years. A total of 420 consecutive patients undergoing AT ablation after previous cardiac interventions (mean 2.1 ± 0.1 prior ablation procedures) were analyzed. Safety, as well as acute and mid-term outcomes of AT ablation were compared between 140 patients ≥75 years (mean age 78.1 ± 0.2 years, 22.9% aged ≥80 years (range 80-86 years)) and 280 patients <75 years (mean age 62.2 ± 0.6 years). Patients ≥75 years were more often female (54.3% vs. 38.2%; = 0.0024) and presented with more cardiac comorbidities, including arterial hypertension (85.0% vs. 64.3%; < 0.0001) and coronary artery disease (33.6% vs. 18.2%; = 0.0006). Acute success of AT ablation was reached in 96.4% vs. 97.9% of patients ( = 0.5173). Major complications (1.4% vs. 0.7%; = 0.6035) and duration of hospital stay (2 (IQR 2-4) days vs. 2 (IQR 2-3) days; = 0.9125) did not differ significantly between groups. During a follow-up of 364 (IQR 183-729.5) days, arrhythmia recurrences occurred in 45.0% vs. 49.3% ( = 0.4684), whereas repeat ablation was less frequently performed in patients ≥75 years (25.7% vs. 36.1%; = 0.0361). AT ablation in patients ≥75 years after previous cardiac interventions in tertiary arrhythmia centers is safe and effective. Therefore, AT ablation should not be ruled out in elderly patients due to age alone, but should be considered based on arrhythmia burden, symptom severity and concomitant clinical and procedural risk factors.
年龄是心房心律失常发生的一个相关风险因素,也是心血管不良结局的独立预测因子。已知房性心动过速(AT)的发生率会随着年龄增长而增加,但迄今为止,尚无关于老年AT患者的数据。因此,我们试图评估≥75岁患者与<75岁患者相比,AT消融的安全性和结局。分析了420例在先前心脏干预后接受AT消融的连续患者(平均先前消融手术2.1±0.1次)。比较了140例≥75岁患者(平均年龄78.1±0.2岁,22.9%年龄≥80岁(范围80 - 86岁))和280例<75岁患者(平均年龄62.2±0.6岁)AT消融的安全性以及急性和中期结局。≥75岁的患者女性比例更高(54.3%对38.2%;P = 0.0024),且存在更多心脏合并症,包括动脉高血压(85.0%对64.3%;P < 0.0001)和冠状动脉疾病(33.6%对18.2%;P = 0.0006)。AT消融的急性成功率在患者中分别为96.4%和97.9%(P = 0.5173)。主要并发症(1.4%对0.7%;P = 0.6035)和住院时间(2(四分位间距2 - 4)天对2(四分位间距2 - 3)天;P = 0.9125)在两组间无显著差异。在364(四分位间距183 - 729.5)天的随访期间,心律失常复发率分别为45.0%和49.3%(P = 0.4684),而≥75岁患者进行再次消融的频率较低(25.7%对36.1%;P = 0.0361)。在三级心律失常中心,先前有心脏干预的≥75岁患者进行AT消融是安全有效的。因此,不应仅因年龄而排除老年患者进行AT消融,而应根据心律失常负荷、症状严重程度以及伴随的临床和手术风险因素来考虑。