Sukumar Aiswarya, Zaman Shafquat, Mostafa Omar E S, Patel Jamie, Akingboye Akinfemi, Waterland Peter
Department of General and Colorectal Surgery, Royal Devon and Exeter Hospital, Royal Devon University Healthcare NHS Foundation Trust, Exeter, Devon, UK.
Department of General and Colorectal Surgery, Queen's Hospital Burton, University Hospitals of Derby and Burton NHS Foundation Trust, Burton on Trent, Derby, UK.
Langenbecks Arch Surg. 2025 Feb 13;410(1):68. doi: 10.1007/s00423-025-03642-7.
Accurate staging of distal colorectal cancers is paramount in guiding neoadjuvant therapy, peri-operative, and ostomy planning. Early colonic lesions can be difficult to visualise on computed tomography (CT) scans, with tumour location solely deduced via endoscopy with the potential for introducing error. We aimed to address the paucity in literature in this area and assessed the accuracy of radiological and endoscopic localisation of distal colorectal cancers.
Retrospective analysis of an electronic database of patients at a large District General Hospital (DGH) diagnosed with distal colorectal cancer between January 2014 to January 2023 was performed. Patient demographics, investigations, endoscopic, and operative findings were analysed. Outcomes were assessed to determine disparities between pre-operative endoscopy and final tumour location.
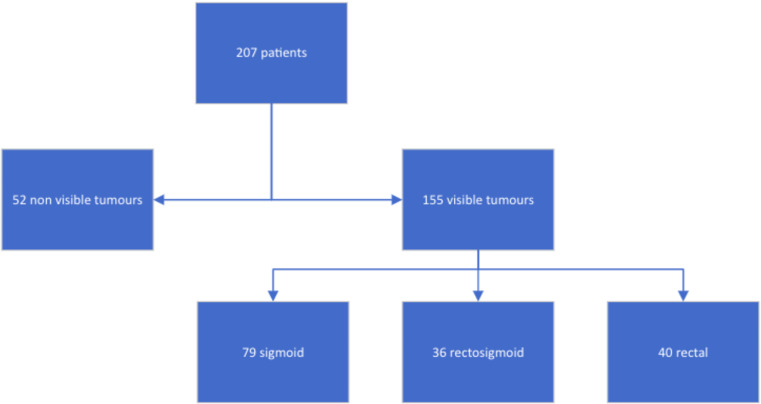
A total of 212 patients were endoscopically diagnosed with distal sigmoid tumour. Of these, 207 (97.6%) had a CT scan performed with 25.1% (52/207) lesions not being identified on this imaging modality with the remainder (74.9%; 155/207) being reported as visible. 38.2% (79/207) of tumours were in the sigmoid colon, 17.4% (36/207) rectosigmoid, and 19.3% (40/207) in the rectum. Pre-operative magnetic resonance imaging (MRI) was performed in 42.5% (90/212) of cases showing 84 tumours: 6.0% (5/84) sigmoid colon, 9.5% (8/84) rectosigmoid and 83.3% (70/84) rectal cancers (upper: 34, mid-rectum: 26, low: 10), with one anal cancer. 42.3% (22/52) of patients with non-visible lesions on CT had MRI scans: 68.2% (15/22) had rectal cancer (upper: 10, mid-rectum: 4, low: 1). Of the 30 where MRI was not performed, 46.7% (14) had sigmoid cancer, 16.7% (5) rectosigmoid, and 33.3% (10) rectal intraoperatively. Overall, 30.7% (65/212) of patients reported as having a distal sigmoid lesion endoscopically in fact had rectal cancer intra-operatively (rectosigmoid lesions excluded).
Endoscopic localisation of distal colorectal tumours can be unreliable for accurate staging and operative planning. A pre-operative MRI scan should be considered in such instances, and particularly for non-visible lesions on CT scan. This may improve peri-operative planning, staging accuracy and patient outcomes.
准确对远端结直肠癌进行分期对于指导新辅助治疗、围手术期及造口术规划至关重要。早期结肠病变在计算机断层扫描(CT)上可能难以显影,肿瘤位置仅通过内镜检查推断,存在引入误差的可能性。我们旨在填补该领域文献的空白,并评估远端结直肠癌的放射学和内镜定位准确性。
对一家大型区综合医院(DGH)2014年1月至2023年1月期间诊断为远端结直肠癌的患者电子数据库进行回顾性分析。分析患者的人口统计学资料、检查、内镜及手术结果。评估结果以确定术前内镜检查与最终肿瘤位置之间的差异。
共有212例患者经内镜诊断为乙状结肠远端肿瘤。其中,207例(97.6%)进行了CT扫描,25.1%(52/207)的病变在该影像学检查中未被发现,其余(74.9%;155/207)被报告为可见。38.2%(79/207)的肿瘤位于乙状结肠,17.4%(36/207)位于直肠乙状结肠交界处,19.3%(40/207)位于直肠。42.5%(90/212)的病例进行了术前磁共振成像(MRI)检查,显示84个肿瘤:6.0%(5/84)位于乙状结肠,9.5%(8/84)位于直肠乙状结肠交界处,83.3%(70/84)位于直肠癌(上段:34例,直肠中段:26例,下段:10例),1例为肛管癌。CT上病变不可见的患者中有42.3%(22/52)进行了MRI扫描:68.2%(15/22)为直肠癌(上段:10例,直肠中段:4例,下段:1例)。在未进行MRI检查的30例患者中,46.7%(14例)术中为乙状结肠癌,16.7%(5例)为直肠乙状结肠交界处癌,33.3%(10例)为直肠癌。总体而言,内镜检查报告为乙状结肠远端病变的患者中,实际上有30.7%(65/212)术中为直肠癌(排除直肠乙状结肠交界处病变)。
远端结直肠肿瘤的内镜定位对于准确分期和手术规划可能不可靠。在这种情况下,应考虑进行术前MRI扫描,特别是对于CT扫描上不可见的病变。这可能会改善围手术期规划、分期准确性和患者预后。