Silverberg Jonathan I, Bieber Thomas, Paller Amy S, Beck Lisa, Kamata Masahiro, Puig Luis, Wiseman Marni, Ezzedine Khaled, Irvine Alan D, Foley Peter, Del Rosso James, Gold Linda Stein, Johansson Erin, Dossenbach Martin, Gallo Gaia, Akmaz Buelent, Casillas Marta, Karlsson Andrei, Curteis Tristan, Chovatiya Raj
Department of Dermatology, The George Washington University School of Medicine and Health Sciences, Washington, USA.
Medicine Campus Davos, Davos, Switzerland.
Dermatol Ther (Heidelb). 2025 Mar;15(3):615-633. doi: 10.1007/s13555-025-01357-7. Epub 2025 Feb 14.
A systematic literature review and network meta-analysis (NMA) were conducted to compare the short-term efficacy of lebrikizumab to other biologic and Janus kinase (JAK) inhibitor monotherapies approved for moderate-to-severe atopic dermatitis in adults and adolescents.
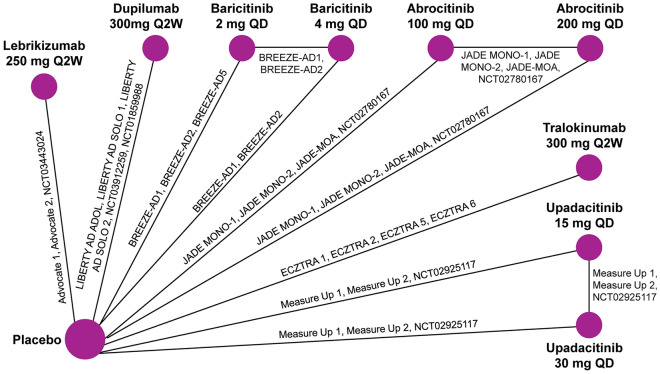
The NMA included randomized, double-blind, placebo-controlled monotherapy phase 2 and 3 trials of biologics (lebrikizumab 250 mg every 2 weeks [Q2W], dupilumab 300 mg Q2W, and tralokinumab 300 mg Q2W) and JAK inhibitors (abrocitinib 100/200 mg daily, baricitinib 2/4 mg daily, and upadacitinib 15/30 mg daily) at approved doses. Efficacy outcomes included the proportions of patients achieving Eczema Area and Severity Index (EASI) improvement, an Investigator Global Assessment of 0 or 1 (IGA 0/1), and a ≥ 4-point improvement in pruritus/itch numeric rating scale score at 12 weeks (abrocitinib) or 16 weeks (other treatments). Itch was also assessed at week 4. A Bayesian NMA employing baseline risk-adjusted random effects models was used to estimate treatment differences.
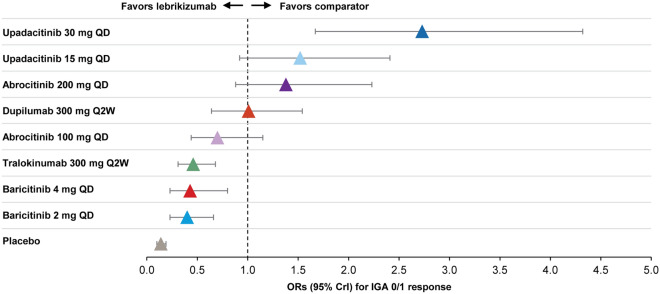
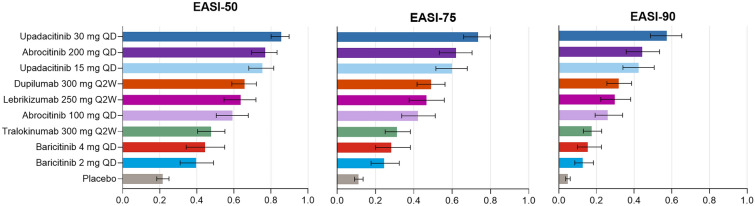
Twenty-two monotherapy studies involving 8531 patients were included in the NMA. By week 12/16, lebrikizumab had superior odds of achieving IGA 0/1 and itch improvement compared to baricitinib and tralokinumab; similar odds to dupilumab, abrocitinib, and upadacitinib 15 mg; and inferior odds to upadacitinib 30 mg. Additionally, lebrikizumab had a higher probability of improving EASI than baricitinib 2 mg; similar probability to baricitinib 4 mg, tralokinumab, dupilumab, abrocitinib, and upadacitinib 15 mg; and lower probability than upadacitinib 30 mg daily. At week 4, lebrikizumab had superior odds of improving itch compared to tralokinumab; similar odds to baricitinib, dupilumab, and abrocitinib 100 mg; and inferior odds to abrocitinib 200 mg and upadacitinib.
Among biologics, lebrikizumab was comparable to dupilumab and superior to tralokinumab in improving response rates at week 16. Upadacitinib 30 mg was the only JAK inhibitor with superior response rates compared to lebrikizumab.
进行了一项系统文献综述和网状Meta分析(NMA),以比较瑞莎珠单抗与其他已获批用于成人和青少年中重度特应性皮炎的生物制剂及Janus激酶(JAK)抑制剂单药疗法的短期疗效。
该NMA纳入了生物制剂(每2周一次250mg瑞莎珠单抗、每2周一次300mg度普利尤单抗和每2周一次300mg曲罗芦单抗)以及JAK抑制剂(每日100/200mg阿布昔替尼、每日2/4mg巴瑞替尼和每日15/30mg乌帕替尼)经批准剂量的随机、双盲、安慰剂对照单药治疗2期和3期试验。疗效指标包括达到湿疹面积和严重程度指数(EASI)改善的患者比例、研究者整体评估为0或1(IGA 0/1)以及在12周(阿布昔替尼)或16周(其他治疗)时瘙痒/瘙痒数字评定量表评分改善≥4分。在第4周时也评估了瘙痒情况。采用基于基线风险调整的随机效应模型的贝叶斯NMA来估计治疗差异。
NMA纳入了涉及8531例患者的22项单药治疗研究。到第12/16周时,与巴瑞替尼和曲罗芦单抗相比,瑞莎珠单抗达到IGA 0/1和瘙痒改善的优势更高;与度普利尤单抗、阿布昔替尼和15mg乌帕替尼相似;但低于30mg乌帕替尼。此外,瑞莎珠单抗改善EASI的概率高于2mg巴瑞替尼;与4mg巴瑞替尼、曲罗芦单抗、度普利尤单抗、阿布昔替尼和15mg乌帕替尼相似;但低于每日30mg乌帕替尼。在第4周时,与曲罗芦单抗相比,瑞莎珠单抗改善瘙痒的优势更高;与巴瑞替尼、度普利尤单抗和100mg阿布昔替尼相似;但低于200mg阿布昔替尼和乌帕替尼。
在生物制剂中,瑞莎珠单抗在第16周改善缓解率方面与度普利尤单抗相当且优于曲罗芦单抗。30mg乌帕替尼是唯一一种与瑞莎珠单抗相比缓解率更高的JAK抑制剂。