The George Washington University School of Medicine and Health Sciences, Washington, DC, USA.
Bispebjerg Hospital, University of Copenhagen, Copenhagen, Denmark.
J Eur Acad Dermatol Venereol. 2021 Sep;35(9):1797-1810. doi: 10.1111/jdv.17351. Epub 2021 Jun 12.
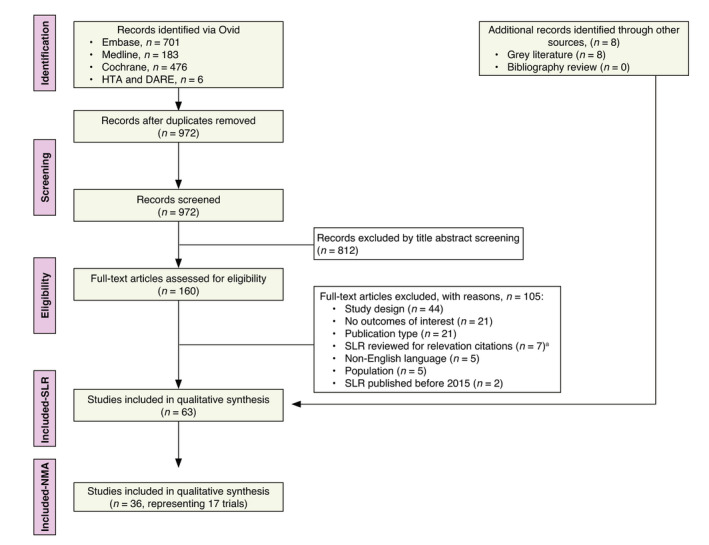
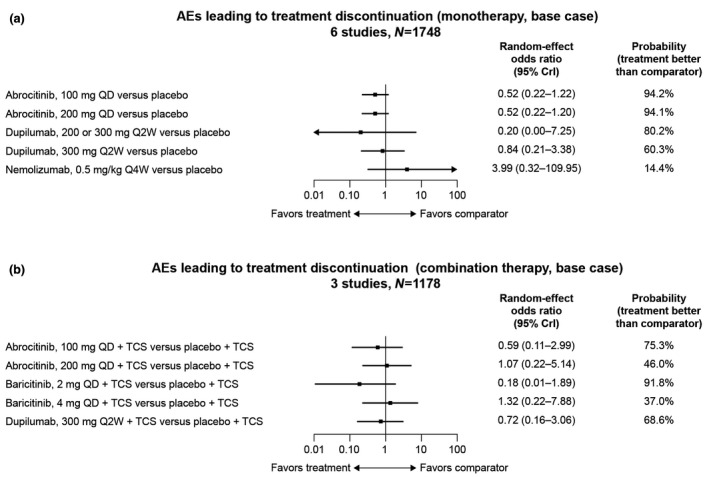
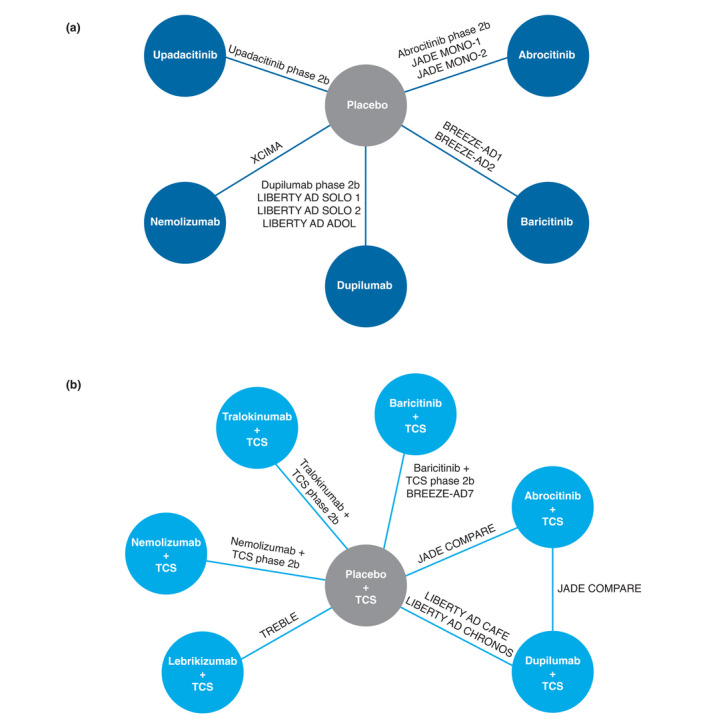
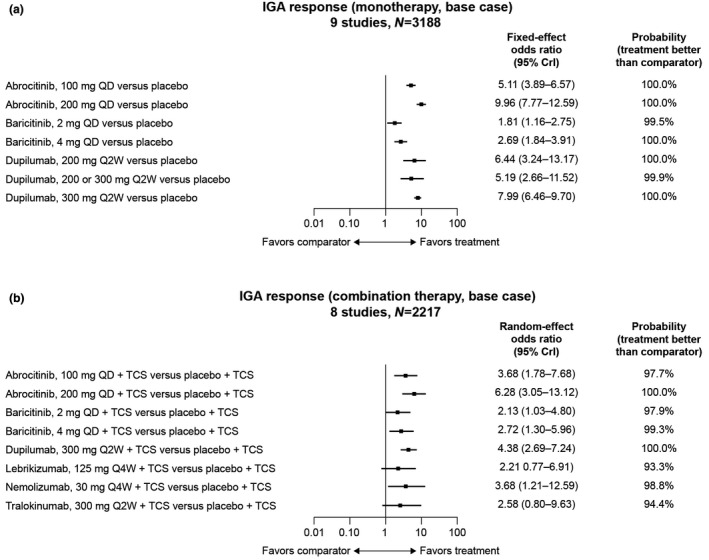
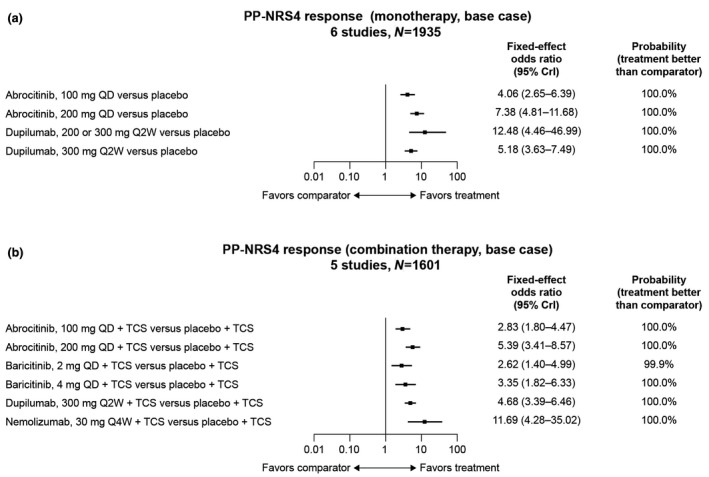
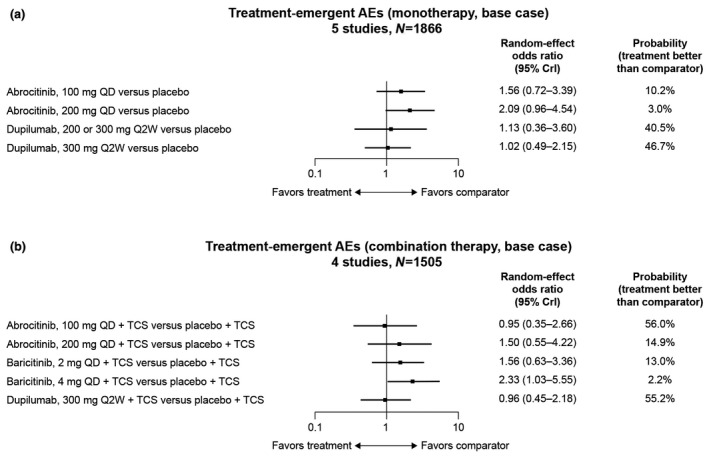
Given the lack of head-to-head studies of systemic therapies in moderate-to-severe atopic dermatitis (AD), network meta-analyses (NMAs) can provide comparative efficacy and safety data to inform clinical decision-making. In this NMA, eligible randomized controlled trials (RCTs) published before 24 October 2019 were identified by a systematic literature review. Short-term (12-16 weeks) efficacy (Investigator's Global Assessment [IGA] and Eczema Area and Severity Index [EASI] responses), patient-reported outcomes (PROs) and safety data from each trial were abstracted and analysed separately for monotherapy and combination therapy (systemic plus topical anti-inflammatory therapy). RCTs were analysed in fixed-effects and random-effects Bayesian NMA models. Overall, 19 phase 2 and phase 3 RCTs of abrocitinib, baricitinib, dupilumab, lebrikizumab, nemolizumab, tralokinumab and upadacitinib were included. In monotherapy RCTs, upadacitinib 30 mg once daily (QD) had the numerically highest efficacy (83.6% achieved ≥50% improvement in EASI [EASI-50 response]), followed by abrocitinib 200 mg QD (74.6%), upadacitinib 15 mg QD (70.5%), dupilumab 300 mg every 2 weeks (Q2W) (63.4%) and abrocitinib 100 mg QD (56.7%). Similar trends in EASI-75 and EASI-90 response were observed. In combination therapy RCTs, abrocitinib 200 mg QD had the highest EASI-50 (86.6%), followed by dupilumab 300 mg Q2W (82.4%) and abrocitinib 100 mg QD (79.7%). Similar findings were observed for IGA response and PROs. In monotherapy and combination therapy RCTs, the probability of treatment-emergent adverse events (TEAEs) was higher among all active treatments than with placebo (except for dupilumab 300 mg Q2W [odds ratio (OR), 0.96; 95% credible interval (CrI), 0.45-2.18] and abrocitinib 100 mg QD [OR, 0.95; 95% CrI, 0.35-2.66] in combination therapy RCTs), although active treatments did not significantly differ from one another. Abrocitinib, dupilumab and upadacitinib were consistently the most effective systemic therapies in adult and adolescent patients with AD, with no significant TEAE differences in short-term RCTs.
鉴于中重度特应性皮炎(AD)系统治疗的头对头研究缺乏,网络荟萃分析(NMAs)可以提供比较疗效和安全性数据,为临床决策提供信息。在这项 NMA 中,通过系统文献检索确定了在 2019 年 10 月 24 日之前发表的合格随机对照试验(RCT)。从每项试验中单独提取并分析短期(12-16 周)疗效(研究者全球评估[IGA]和湿疹面积和严重程度指数[EASI]反应)、患者报告结局(PROs)和安全性数据,分别用于单药治疗和联合治疗(全身加局部抗炎治疗)。RCT 采用固定效应和随机效应贝叶斯 NMA 模型进行分析。总体而言,纳入了 abrocitinib、baricitinib、dupilumab、lebrikizumab、nemolizumab、tralokinumab 和 upadacitinib 的 19 项 2 期和 3 期 RCT。在单药治疗 RCT 中,upadacitinib 30mg 每日一次(QD)的疗效(EASI-50 应答中 83.6%达到≥50%改善)最高,其次是 abrocitinib 200mg QD(74.6%)、upadacitinib 15mg QD(70.5%)、dupilumab 300mg 每 2 周(Q2W)(63.4%)和 abrocitinib 100mg QD(56.7%)。同样的趋势也观察到 EASI-75 和 EASI-90 应答。在联合治疗 RCT 中,abrocitinib 200mg QD 的 EASI-50 最高(86.6%),其次是 dupilumab 300mg Q2W(82.4%)和 abrocitinib 100mg QD(79.7%)。IGA 反应和 PROs 也观察到类似的结果。在单药和联合治疗 RCT 中,与安慰剂相比,所有活性治疗的治疗出现不良事件(TEAEs)的概率均高于安慰剂(dupilumab 300mg Q2W 除外[比值比(OR),0.96;95%可信区间(CrI),0.45-2.18]和 abrocitinib 100mg QD [OR,0.95;95% CrI,0.35-2.66]在联合治疗 RCT 中),尽管活性治疗彼此之间没有显著差异。阿巴西普、度普利尤单抗和 upadacitinib 在成人和青少年 AD 患者中一直是最有效的系统性治疗药物,短期 RCT 中无明显的 TEAE 差异。