Salbach Christian, Yildirim Mustafa, Hund Hauke, Müller-Hennessen Matthias, Frey Norbert, Katus Hugo Anton, Giannitsis Evangelos, Milles Barbara Ruth
Department of Internal Medicine III, Cardiology, University Hospital of Heidelberg, Im Neuenheimer Feld 410, 69120, Heidelberg, Germany.
BMC Emerg Med. 2025 Mar 3;25(1):35. doi: 10.1186/s12873-025-01194-z.
Evidence suggests a benefit of a rhythm control approach in patients with a recent diagnosis of atrial fibrillation (AF). This study sought to evaluate clinical characteristics, treatment strategies and outcomes in patients with first diagnosed AF (FDAF) undergoing a non-invasive rhythm control strategy in an emergency department (ED).
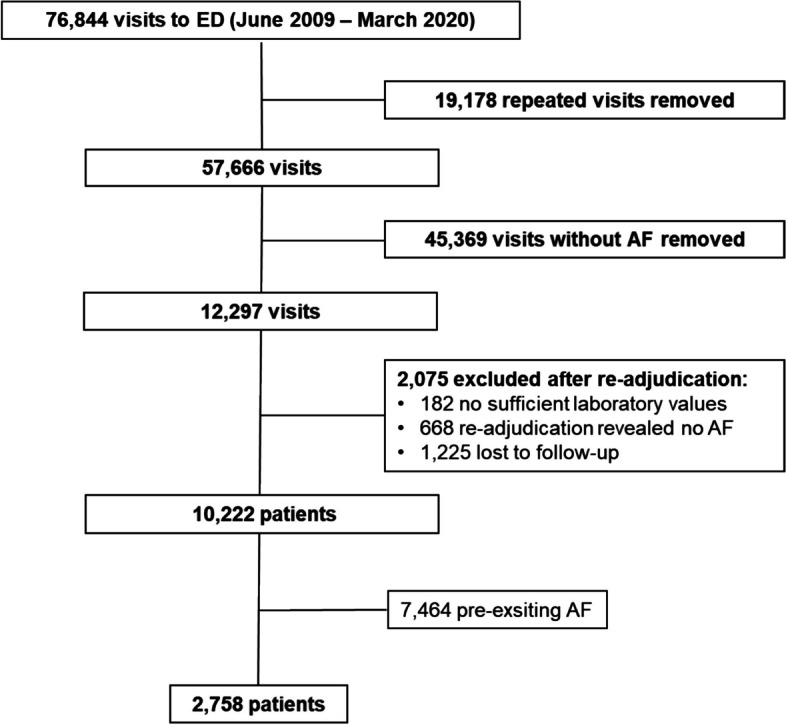
This analysis uses data from the Heidelberg Registry of Atrial Fibrillation (HERA-FIB). HERA-FIB is a retrospective single-centre observational study which consecutively included patients presenting to the ED of the University Hospital of Heidelberg between June 2009 and March 2020 with a sequential follow-up for all-cause mortality, stroke, major bleeding events and myocardial infarction (MI). Outcomes of patients with FDAF were related to treatment strategy (non-invasive rhythm vs. rate control).
Among the 2,758 (27%) patients who presented with FDAF, a non-implementation of a non-invasive rhythm control strategy at admission was observed in 75.4% and associated with an excess of all-cause mortality hazard ratio (HR): 1.61 (95%CI 1.30-1.99), p < 0.0001 and incident MI HR: 1.88 (95% CI 1.22-2.90), p = 0.0043 during follow-up. The non-implementation of a non-invasive rhythm control remained an independent predictor for all-cause mortality and MI even after adjustment for significant univariate variables with an adjusted HR of 1.52 (95%CI: 1.14-2.04, p = 0.0043) and 1.89 (95%CI: 1.03-3.45, p = 0.0392), respectively.
Real-world data from FDAF patients presenting to an ED showed a benefit regarding all-cause mortality and MI favouring a non-invasive rhythm control strategy. Further prospective research is needed to validate this hypothesis.
The trial was registered at ClinicalTrials.gov Identifier: NCT05995561.
有证据表明,对于近期诊断为心房颤动(AF)的患者,节律控制方法有益。本研究旨在评估在急诊科(ED)接受非侵入性节律控制策略的初诊房颤(FDAF)患者的临床特征、治疗策略和结局。
本分析使用来自海德堡心房颤动登记处(HERA-FIB)的数据。HERA-FIB是一项回顾性单中心观察性研究,连续纳入2009年6月至2020年3月期间到海德堡大学医院急诊科就诊的患者,并对全因死亡率、中风、大出血事件和心肌梗死(MI)进行序贯随访。FDAF患者的结局与治疗策略(非侵入性节律控制与心率控制)相关。
在2758例(27%)表现为FDAF的患者中,75.4%的患者在入院时未实施非侵入性节律控制策略,这与全因死亡率风险比(HR)过高相关:1.61(95%CI 1.30 - 1.99),p < 0.0001,以及随访期间新发MI的HR:1.88(95%CI 1.22 - 2.90),p = 0.0043。即使在对显著的单变量进行调整后,未实施非侵入性节律控制仍然是全因死亡率和MI的独立预测因素,调整后的HR分别为1.52(95%CI:1.14 - 2.04,p = 0.0043)和1.89(95%CI:1.03 - 3.45,p = 0.0392)。
来自到急诊科就诊的FDAF患者的真实世界数据显示,在全因死亡率和MI方面,非侵入性节律控制策略具有优势。需要进一步的前瞻性研究来验证这一假设。
该试验在ClinicalTrials.gov注册,标识符:NCT05995561。