Ron Donna, Daley Alton B, Coe Marcus P, Herrick Michael D, Roth Robert H, Abess Alexander T, Martinez-Camblor Pablo, Deiner Stacie G, Boone Myles D
Department of Community and Family Medicine, Dartmouth Hitchcock Medical Center, Lebanon, NH, Geisel School of Medicine at Dartmouth, Hanover, NH; Department of Anesthesiology, Critical Care, and Pain Medicine, Meir Medical Center and Tel Aviv University, 59 Tchernichovsky St, Kefar Sava 4428164, Israel.
Department of Orthopaedic Surgery, Dartmouth Hitchcock Medical Center, Lebanon, NH, Geisel School of Medicine at Dartmouth, Hanover, NH.
J Frailty Aging. 2025 Apr;14(2):100030. doi: 10.1016/j.tjfa.2025.100030. Epub 2025 Mar 5.
Major joint surgery is one of the largest components of Medicare spending in the US and the most frequent major procedure performed in older adults. Increasing age is associated with increasing prevalence of frailty, but the influence of frailty on healthcare expenditures following arthroplasty has yet to be adequately explored.
To explore the association between frailty and healthcare expenditures in the year following total hip and knee arthroplasties.
Retrospective cohort study SETTING: United States population PARTICIPANTS: Medicare beneficiaries 65 and older undergoing total knee or hip arthroplasty (n = 1,152,872) from 2017 through 2018.
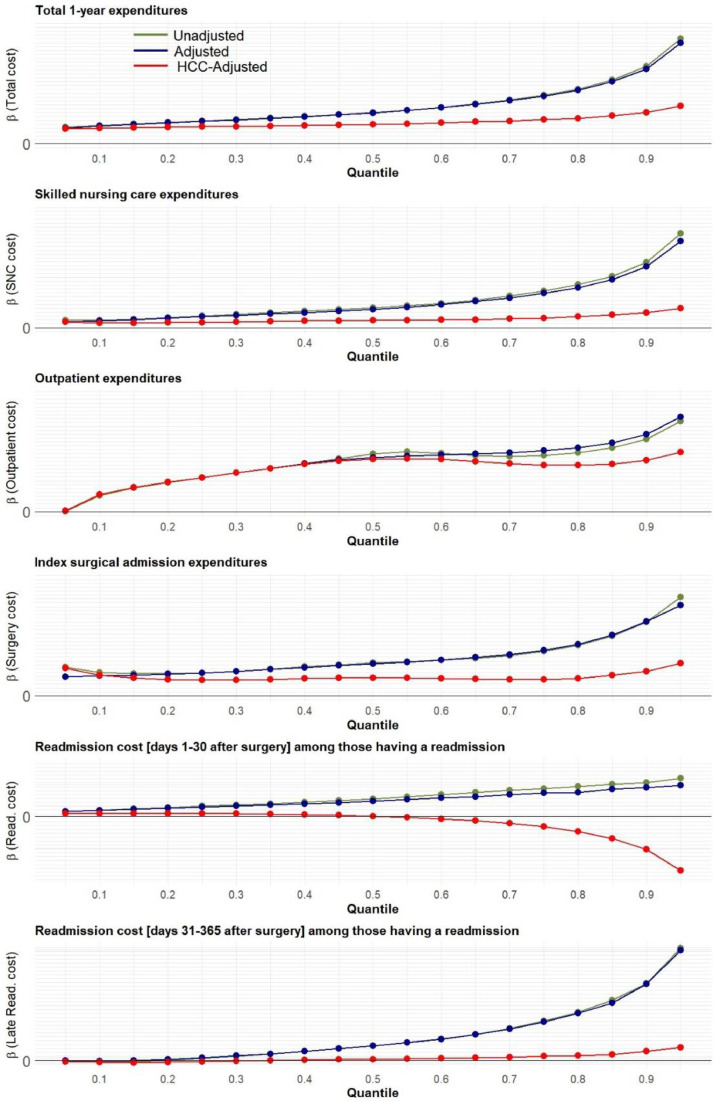
Claims-based frailty index (exposure), total 1-year Medicare expenditures broken down by category (primary outcome), in-hospital complications, length of stay, discharge destination, readmission and mortality (secondary outcomes).
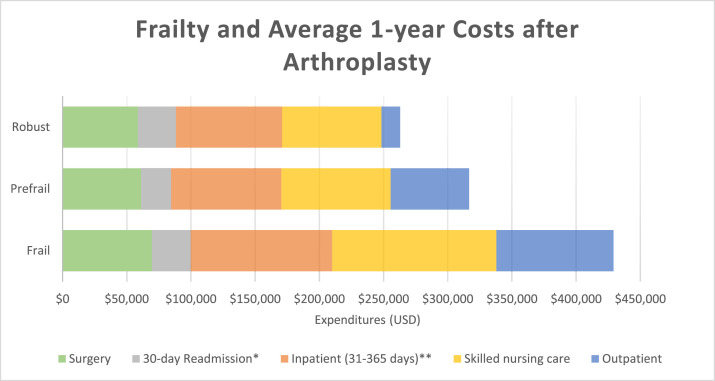
Among 435,496 patients who underwent hip (37.8 %) and 717,376 patients who underwent knee arthroplasty (62.2 %), the mean age was 73.7 years and 19.2 % were classified as frail. Median total expenditures in US dollars at one year were higher in those with frailty ($247,503; IQR [$169,400-$391,176]) relative to the prefrail ($179,379 [$127,396-$265,039]) and robust ($130,314 [$85,438-$199,605]) groups. Total expenditures included the index surgical admission, rehospitalization, skilled nursing care, and outpatient care, all of which were higher with increasing frailty. However, the surgical procedure accounted for less than a third of the total 1-year healthcare costs and was the category with the lowest degree of variation between patients. Frailty was also associated with longer lengths of stay, higher risks of complications, readmission, and mortality and lower likelihood of being discharged home after the procedure.
Among older adults undergoing total hip and knee arthroplasty, frailty is associated with higher healthcare expenditures, predominantly driven by longitudinal care during the year following the procedure. More research is needed to test interventions to improve outcomes and reduce cost in this high-risk population.
在美国,大型关节手术是医疗保险支出的最大组成部分之一,也是老年人最常进行的大型手术。年龄增长与虚弱患病率增加相关,但虚弱对关节置换术后医疗保健支出的影响尚未得到充分探讨。
探讨全髋关节和膝关节置换术后一年内虚弱与医疗保健支出之间的关联。
回顾性队列研究
美国人群
2017年至2018年接受全膝关节或髋关节置换术的65岁及以上医疗保险受益人(n = 1,152,872)。
基于索赔的虚弱指数(暴露因素)、按类别细分的1年医疗保险总支出(主要结局)、住院并发症、住院时间、出院目的地、再入院和死亡率(次要结局)。
在接受髋关节置换术的435,496例患者(37.8%)和接受膝关节置换术的717,376例患者(62.2%)中,平均年龄为73.7岁,19.2%被归类为虚弱。与非虚弱组(179,379美元[127,396 - 265,039美元])和健康组(130,314美元[85,438 - 199,605美元])相比,虚弱组一年的总支出中位数(247,503美元;四分位间距[169,400 - 391,176美元])更高。总支出包括首次手术入院、再次住院、专业护理和门诊护理,所有这些随着虚弱程度的增加而增加。然而,手术费用占1年医疗保健总成本的不到三分之一,并且是患者之间差异程度最低的类别。虚弱还与更长的住院时间、更高的并发症、再入院和死亡风险以及术后出院回家的可能性较低相关。
在接受全髋关节和膝关节置换术的老年人中,虚弱与更高的医疗保健支出相关,主要由术后一年的长期护理驱动。需要更多研究来测试干预措施,以改善这一高风险人群的结局并降低成本。