Hu Anquan, Zhang Kun, Sun Wei, Li Xian, Zhou Lianwan, Li Xi, Chen Feng, Liu Tao
Geriatric Center, Hainan General Hospital (Hainan Affiliated Hospital of Hainan Medical University), Haikou, 570311, China.
Department of Neurology, Hainan General Hospital (Hainan Affiliated Hospital of Hainan Medical University), Haikou, 570311, China.
Lipids Health Dis. 2025 Mar 6;24(1):83. doi: 10.1186/s12944-025-02501-0.
The neutrophil-to-high-density lipoprotein cholesterol ratio (NHR) has emerged as a potential biomarker for chronic disease outcomes. Cognitive impairment is a major contributor to mortality in older adults. However, the combined effect of NHR and cognitive function on all-cause mortality remains unclear. This study aims to investigate the joint impact of NHR and cognitive impairment on all-cause mortality in this population.
We analyzed participants in the National Health and Nutrition Examination Survey (NHANES) between 2011 and 2014. Participants were grouped according to NHR levels, DSST scores, and the combined NHR and DSST. Weighted Cox regression models assessed the association between NHR, cognitive impairment, and all-cause mortality. Weighted Kaplan-Meier curves estimated survival probabilities.
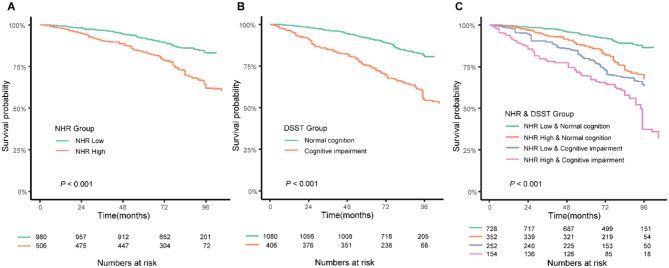
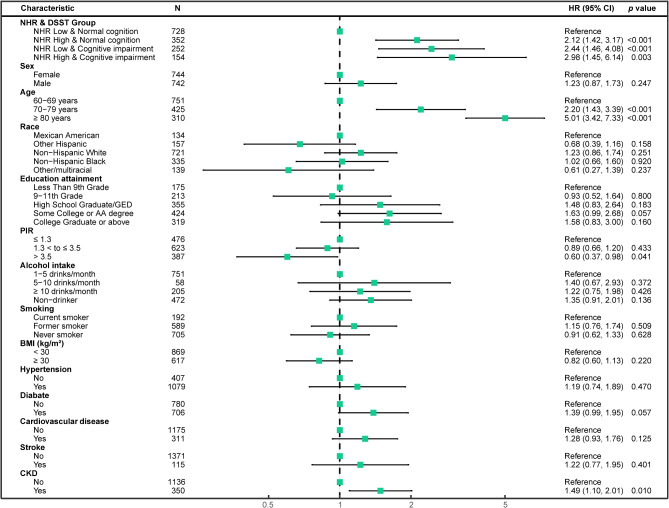
The study involved 1,486 participants (weighted sample was 54,078,084) aged 60 years and older, of whom 81.76% (n = 1,180) survived and 18.24% (n = 306) died by the end of follow-up. The median follow-up time was 78 months (IQR: 68-94). Weighted multivariable Cox regression revealed that high NHR (HR = 1.82, 95% CI: 1.21-2.74; P = 0.004), cognitive impairment (HR = 1.87, 95% CI: 1.25-2.79; P = 0.002), and the combination of high NHR and cognitive impairment (HR = 2.98, 95% CI: 1.45-6.14; P = 0.003) were independently associated with higher all-cause mortality, after full adjustment in model 3. Kaplan-Meier curves revealed significant survival differences, with the highest survival rate in the NHR Low & Normal cognition and the lowest in the NHR High & Cognitive impairment (P < 0.001).
High NHR and cognitive impairment in aged 60 years and older have an increased risk of all-cause mortality. These findings underscore the importance of integrating both NHR and cognitive assessments in mortality risk evaluations, offering a potential strategy for early intervention in aging populations.
中性粒细胞与高密度脂蛋白胆固醇比值(NHR)已成为慢性疾病预后的一种潜在生物标志物。认知障碍是老年人死亡的主要原因。然而,NHR与认知功能对全因死亡率的综合影响仍不明确。本研究旨在调查NHR和认知障碍对该人群全因死亡率的联合影响。
我们分析了2011年至2014年美国国家健康与营养检查调查(NHANES)的参与者。参与者根据NHR水平、数字符号替换测验(DSST)得分以及NHR与DSST的组合进行分组。加权Cox回归模型评估NHR、认知障碍与全因死亡率之间的关联。加权Kaplan-Meier曲线估计生存概率。
该研究纳入了1486名60岁及以上的参与者(加权样本为54,078,084),其中81.76%(n = 1180)在随访结束时存活,18.24%(n = 306)死亡。中位随访时间为78个月(四分位间距:68 - 94)。加权多变量Cox回归显示,高NHR(HR = 1.82,95%置信区间:1.21 - 2.74;P = 0.004)、认知障碍(HR = 1.87,95%置信区间:1.25 - 2.79;P = 0.002)以及高NHR与认知障碍的组合(HR = 2.98,95%置信区间:1.45 - 6.14;P = 0.003)在模型3进行全面调整后与较高的全因死亡率独立相关。Kaplan-Meier曲线显示出显著的生存差异,NHR低且认知正常组的生存率最高,NHR高且认知障碍组的生存率最低(P < 0.001)。
60岁及以上人群中高NHR和认知障碍会增加全因死亡率风险。这些发现强调了在死亡风险评估中综合NHR和认知评估的重要性,为老年人群的早期干预提供了一种潜在策略。