Tapiainen Vilja V, Sirniö Päivi, Elomaa Hanna, Karjalainen Henna, Äijälä Ville K, Kastinen Meeri, Kehusmaa Akseli, Pohjanen Vesa-Matti, Lindgren Outi, Sirkiä Onni, Ahtiainen Maarit, Helminen Olli, Wirta Erkki-Ville, Rintala Jukka, Saarnio Juha, Rautio Tero, Seppälä Toni T, Böhm Jan, Mecklin Jukka-Pekka, Tuomisto Anne, Mäkinen Markus J, Väyrynen Juha P
Translational Medicine Research Unit, Medical Research Center Oulu, Oulu University Hospital, and University of Oulu, Oulu, Finland.
Department of Biological and Environmental Science, University of Jyväskylä, Jyväskylä, Finland.
Br J Cancer. 2025 May;132(9):805-813. doi: 10.1038/s41416-025-02972-z. Epub 2025 Mar 7.
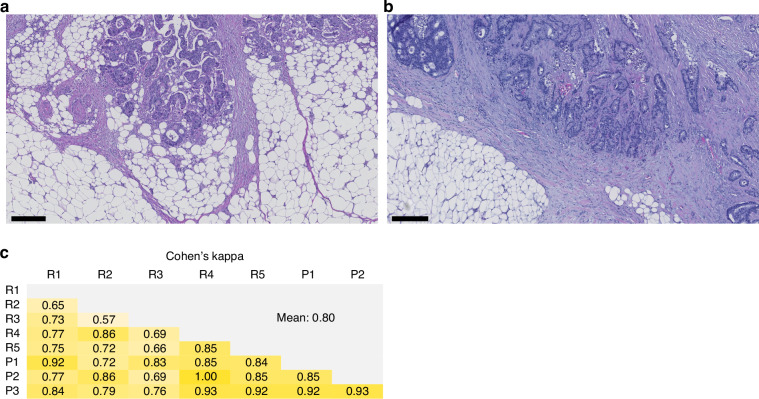
SARIFA (Stroma AReactive Invasion Front Areas), defined as the direct contact between a tumour cell cluster and adipose cells at the invasion margin, has been proposed as a prognostic marker in gastrointestinal cancers. We hypothesized that SARIFA is associated with an immunosuppressive tumour microenvironment.
SARIFA status was evaluated in two large colorectal cancer cohorts (N = 1876). Survival analyses were performed using multivariable Cox regression. Immune cell densities were analysed utilizing multiplex and conventional immunohistochemistry combined with digital image analysis.
SARIFA-positivity was independently associated with a shorter cancer-specific survival in both cohorts [Cohort 1: hazard ratio (HR) for SARIFA-positive (vs. negative) 1.75 (95% CI 1.35-2.25), P < 0.0001; Cohort 2: HR for SARIFA-positive (vs. negative) 2.09 (95% CI 1.43-3.05), P = 0.0001]. SARIFA-positivity was associated with lower densities of CD3 T cells, CD66b granulocytes, M1-like macrophages, and CD14HLA-DR mature monocytic cells, but higher densities of M2-like macrophages and CD14HLA-DR immature monocytic cells. Mean Cohen's kappa for SARIFA evaluation between eight investigators was 0.80.
SARIFA status is a highly reproducible, independent prognostic factor in colorectal cancer. SARIFA-positivity is associated with lower densities of antitumourigenic immune cells and the polarisation of macrophages towards a protumourigenic M2-like phenotype.
SARIFA(基质反应性侵袭前沿区域)被定义为肿瘤细胞簇与侵袭边缘脂肪细胞之间的直接接触,已被提议作为胃肠道癌症的预后标志物。我们假设SARIFA与免疫抑制性肿瘤微环境相关。
在两个大型结直肠癌队列(N = 1876)中评估SARIFA状态。使用多变量Cox回归进行生存分析。利用多重和传统免疫组织化学结合数字图像分析来分析免疫细胞密度。
在两个队列中,SARIFA阳性均与较短的癌症特异性生存期独立相关[队列1:SARIFA阳性(与阴性相比)的风险比(HR)为1.75(95%CI 1.35 - 2.25),P < 0.0001;队列2:SARIFA阳性(与阴性相比)的HR为2.09(95%CI 1.43 - 3.05),P = 0.0001]。SARIFA阳性与CD3 T细胞、CD66b粒细胞、M1样巨噬细胞和CD14HLA - DR成熟单核细胞的密度较低相关,但与M2样巨噬细胞和CD14HLA - DR未成熟单核细胞的密度较高相关。八位研究者之间对SARIFA评估的平均Cohen's kappa为0.80。
SARIFA状态是结直肠癌中高度可重复的独立预后因素。SARIFA阳性与抗肿瘤免疫细胞密度较低以及巨噬细胞向促肿瘤M2样表型的极化相关。