Mvula Mc Geofrey, Aron Moses Banda, Mphande Isaac, Namwali Lemekeza, Nazimera Lawrence, Kusamba Martha, Ndarama Enoch, Sonenthal Paul, Blair Alden Hooper, Baltzell Kimberly, Munyaneza Fabien, Kachimanga Chiyembekezo, Matanje Beatrice, Connolly Emilia
Partners in Health, P. O Box 56, Neno, Malawi.
Neno District Health Office, Ministry of Health, Neno, Malawi.
BMC Pediatr. 2025 Mar 11;25(1):184. doi: 10.1186/s12887-025-05558-z.
Despite efforts to improve neonatal care worldwide, neonatal mortality rates in sub-Saharan Africa remain high. Adequate space, equipment, and staff are vital to improving mortality rates through high-quality care. We evaluated the impact of a district-level neonatal special care nursery over seven years at Neno District Hospital, Malawi.
We conducted a retrospective cohort study to measure the neonatal outcomes in the neonatal special care nursery before nursery establishment (study period I, 2014-2015), following the establishment of a small nursery (study period II, 2016-2018), then with a transition to a larger nursery (study period III, 2019-2021). We extracted data from the neonatal registers and employed descriptive statistics and chi-square tests to compare the overall neonatal outcomes between study periods. We performed logistic regression to isolate factors associated with neonates alive at discharge.
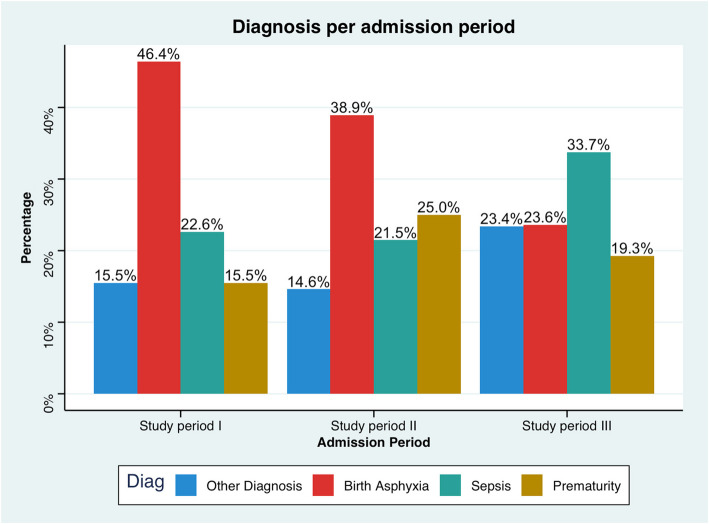
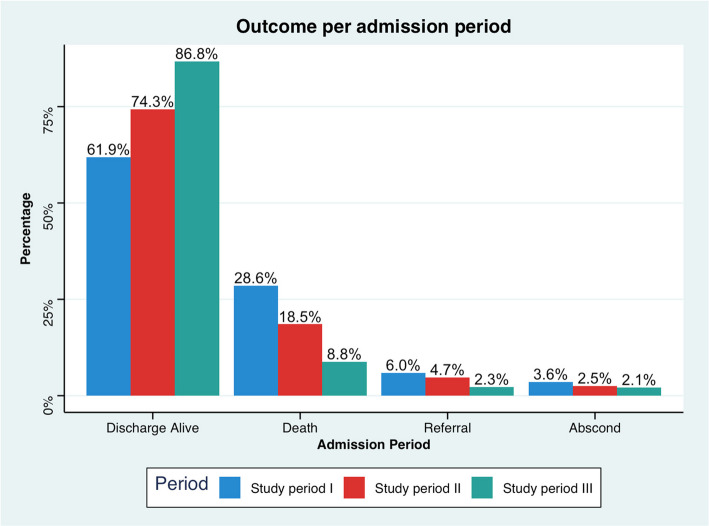
Of the 1366 neonates observed over the entire study period, the three primary admission diagnoses were birth asphyxia (30.1%), sepsis (29.0%), and prematurity (20.9%). The proportion of neonates discharged alive increased from 61.9% to 74.3% and then 87.6% in study periods I, II, and III, respectively. Neonates admitted during study periods II and III were over two and five times more likely to be discharged alive than neonates admitted during study period I in multivariate analysis controlling for sex (SPII aOR = 2.42; 95% CI: 1.43-4.08; SPIII aOR = 5.32; 95% CI: 3.13-8.98; p < 0.001). There was no difference in being discharged alive for neonates admitted with prematurity compared to birth asphyxia (aOR 0.87; 95% CI: 0.51-.151) but neonates admitted with sepsis were over two times more likely to be discharged alive than birth asphyxia (aOR = 2.64; 95% CI: 1.67-4.29). Neonates admitted with a birth weight of 1500 g were 69% less likely to be discharged alive than neonates admitted with a birth weight > 2500 g (aOR = 0.31, 95% CI: 0.16-0.58; p < 0.001).
The establishment and systems strengthening of a neonatal nursery at Neno District Hospital resulted in a significant increase of neonates discharged alive from the neonatal special care nursery. A multidimensional approach to ensuring resource inputs and ongoing strengthening efforts in Malawi is critical to decreasing neonatal mortality within the special care nursery.
尽管全球都在努力改善新生儿护理,但撒哈拉以南非洲地区的新生儿死亡率仍然很高。充足的空间、设备和工作人员对于通过高质量护理提高死亡率至关重要。我们评估了马拉维内诺区医院的区级新生儿特别护理病房在七年中的影响。
我们进行了一项回顾性队列研究,以测量新生儿特别护理病房建立前(研究期I,2014 - 2015年)、小型病房建立后(研究期II,2016 - 2018年)以及过渡到大型病房后(研究期III,2019 - 2021年)的新生儿结局。我们从新生儿登记册中提取数据,并采用描述性统计和卡方检验来比较各研究期之间的总体新生儿结局。我们进行逻辑回归以分离与出院时存活新生儿相关的因素。
在整个研究期间观察的1366例新生儿中,三个主要入院诊断为出生窒息(30.1%)、败血症(29.0%)和早产(20.9%)。存活出院的新生儿比例在研究期I、II和III中分别从61.9%增加到74.3%,然后增加到87.6%。在控制性别的多变量分析中,研究期II和III期间入院的新生儿存活出院的可能性分别是研究期I期间入院新生儿的两倍多和五倍多(SPII调整后比值比 = 2.42;95%置信区间:1.43 - 4.08;SPIII调整后比值比 = 5.32;95%置信区间:3.13 - 8.98;p < 0.)。与出生窒息相比,早产入院的新生儿存活出院没有差异(调整后比值比0.87;95%置信区间:0.51 - 1.151),但败血症入院的新生儿存活出院的可能性是出生窒息的两倍多(调整后比值比 = 2.64;95%置信区间:1.67 - 4.29)。出生体重<1500克的入院新生儿存活出院的可能性比出生体重>2500克的入院新生儿低69%(调整后比值比 = 0.31,95%置信区间:0.16 - 0.58;p < 0.001)。
内诺区医院新生儿病房的建立和系统强化导致新生儿特别护理病房存活出院的新生儿显著增加。在马拉维,采取多维度方法确保资源投入和持续强化努力对于降低特别护理病房内的新生儿死亡率至关重要。