Sawata Tetsuro, Sakamoto Susumu, Usui Yusuke, Suzuki Aika, Kitamura Hideya, Iwasawa Tae, Matsushita Shoichiro, Terasaki Yasuhiro, Kunugi Shinobu, Kishi Kazuma, Fujisawa Tomoyuki, Suda Takafumi, Homma Sakae
Department of Respiratory Medicine, AOI Universal Hospital, Kawasaki, Japan.
Department of Respiratory Medicine, Toho University Graduate School of Medicine, Ōta, Japan.
Clin Respir J. 2025 Mar;19(3):e70061. doi: 10.1111/crj.70061.
Anti-neutrophil cytoplasmic antibody (ANCA) seropositivity strongly correlates to ANCA-associated vasculitis. Patients with idiopathic interstitial pneumonias (IIPs) without systemic vasculitis are sometimes ANCA-positive. Radiological and pathological differences between patients with myeloperoxidase (MPO)-ANCA-positive and those with proteinase 3 (PR3)-ANCA-positive IIPs remain unclear. To determine whether high-resolution computed tomography (HRCT) features and pathology findings differ by ANCA subtype in ANCA-positive IIP patients in a national database. Clinical, radiological, and pathological data were examined along with a web-based multidisciplinary discussion.
We reviewed records of 10 MPO-ANCA-positive and 9 PR3-ANCA-positive IIP patients who underwent HRCT and surgical lung biopsy between April 2009 and March 2014. Pulmonologists, chest radiologists, and pathologists evaluated HRCT scans and pathological findings independently. Patterns were classified using ATS/ERS/JRS/ALAT 2011 guidelines for idiopathic pulmonary fibrosis.
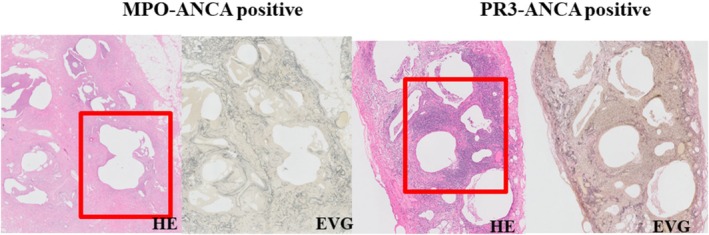
HRCT patterns were definite usual interstitial pneumonia (UIP) (n = 8; 42.1%), possible UIP (n = 6; 31.6%), and inconsistent with UIP (n = 5; 26.3%). Pathological patterns were definite UIP (n = 5; 26.3%), probable UIP (n = 8; 42.1%), possible UIP (n = 4; 21.1%), and not UIP (n = 2; 10.5%). HRCT and pathological patterns did not differ between MPO-ANCA-positive and PR3-ANCA-positive IIPs. Radiological features were reticulation (n = 13; 68.4%), nodules (n = 12; 63.1%), honeycombing (n = 10; 52.6%), and increased attenuation around honeycombing (n = 7; 36.8%). Pathological findings were cysts (n = 12; 63.1%), lymphoid follicles with germinal centers (n = 11; 57.9%), and peribronchiolar wall lymphocytic infiltration (n = 11; 57.9%).
HRCT and pathological patterns did not differ between MPO-ANCA-positive and PR3-ANCA-positive IIPs. This absence of significant differences suggests a similar mechanism underlying both types of interstitial pneumonia.
抗中性粒细胞胞浆抗体(ANCA)血清阳性与ANCA相关性血管炎密切相关。无系统性血管炎的特发性间质性肺炎(IIP)患者有时ANCA呈阳性。髓过氧化物酶(MPO)-ANCA阳性和蛋白酶3(PR3)-ANCA阳性的IIP患者之间的影像学和病理学差异尚不清楚。为了确定国家数据库中ANCA阳性IIP患者的高分辨率计算机断层扫描(HRCT)特征和病理结果是否因ANCA亚型而异。我们对临床、影像学和病理数据进行了检查,并进行了基于网络的多学科讨论。
我们回顾了2009年4月至2014年3月期间接受HRCT和外科肺活检的10例MPO-ANCA阳性和9例PR3-ANCA阳性IIP患者的记录。肺科医生、胸部放射科医生和病理学家分别评估HRCT扫描和病理结果。使用美国胸科学会/欧洲呼吸学会/日本呼吸学会/拉丁美洲胸科协会2011年特发性肺纤维化指南对模式进行分类。
HRCT模式为明确的普通型间质性肺炎(UIP)(n = 8;42.1%)、可能的UIP(n = 6;31.6%)以及与UIP不一致(n = 5;26.3%)。病理模式为明确的UIP(n = 5;26.3%)、可能的UIP(n = 8;42.1%)、可能的UIP(n = 4;21.1%)以及非UIP(n = 2;10.5%)。MPO-ANCA阳性和PR3-ANCA阳性的IIP患者之间的HRCT和病理模式没有差异。影像学特征为网状影(n = 13;68.4%)、结节(n = 12;63.1%)、蜂窝状影(n = 10;52.6%)以及蜂窝状影周围的密度增加(n = 7;36.8%)。病理结果为囊肿(n = 12;63.1%)、有生发中心的淋巴滤泡(n = 11;57.9%)以及细支气管壁淋巴细胞浸润(n = 11;57.9%)。
MPO-ANCA阳性和PR3-ANCA阳性的IIP患者之间的HRCT和病理模式没有差异。这种无显著差异表明两种间质性肺炎的潜在机制相似。