Medina-Gil Daniel, Palomo Laura, Navarro Víctor, Lázaro Gonzalo, Martín-Mur Beatriz, Hernández Cristina, Castells Oriol, Sánchez Belén, Muñoz-Torres Pau Marc, Pagès Carlota, Pujadas Gemma, Esteve-Codina Anna, Cabirta Alba, Ferrà Christelle, Alcoceba Miguel, Terol Maria José, Andreu Rafael, Martí Mercè, Abrisqueta Pau, Bosch Francesc, Crespo Marta
Experimental Hematology, Vall d'Hebron Institute of Oncology (VHIO), Vall d'Hebron Barcelona Hospital Campus, Barcelona, Spain; Department of Medicine, Universitat Autònoma de Barcelona, Bellaterra.
Oncology Data Science (ODysSey) Group, Vall d'Hebron Institute of Oncology (VHIO), Vall d'Hebron Barcelona Hospital Campus, Barcelona.
Haematologica. 2025 Aug 1;110(8):1758-1773. doi: 10.3324/haematol.2024.286663. Epub 2025 Mar 13.
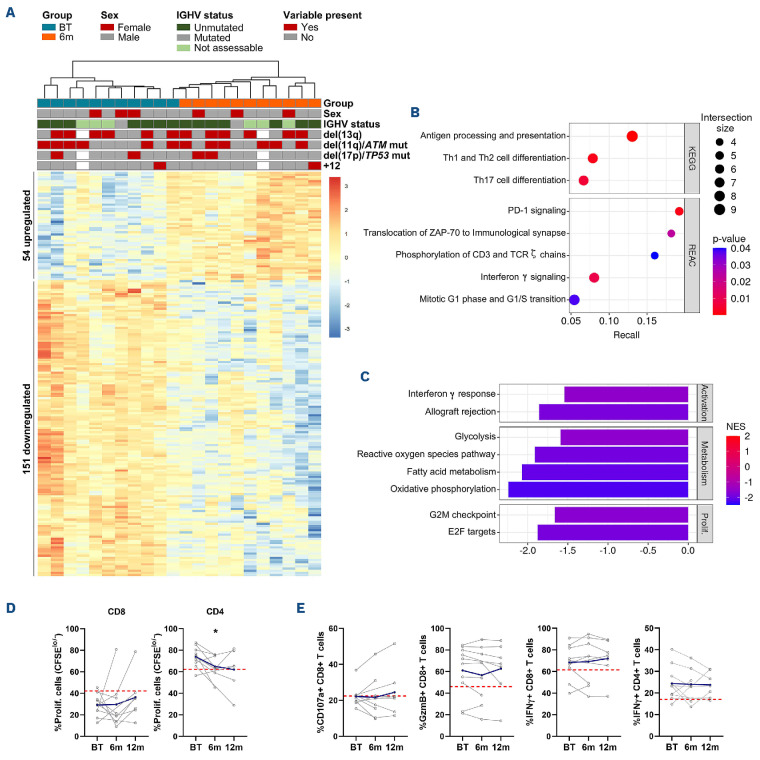
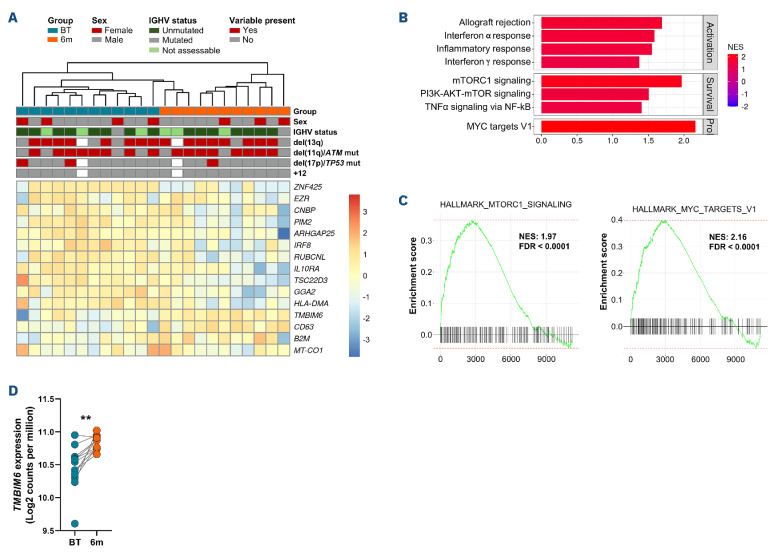
Continuous treatment with ibrutinib not only exerts tumor control but also enhances T-cell function in patients with chronic lymphocytic leukemia (CLL). We conducted longitudinal multi-omics analyses in samples from CLL patients receiving ibrutinib upfront to identify potential adaptive mechanisms to Bruton tyrosine kinase (BTK) inhibition during the first 12 months of continuous therapy. We found that ibrutinib induced a decrease in the expression of exhaustion markers and the proportion of regulatory T cells and T-follicular helper cells normalized to levels observed in healthy donors. Functionally, the expression of genes related to activation, proliferation, differentiation, and metabolism were downregulated in T cells; after in vitro stimulation, proliferation capacity was only slightly modified by ibrutinib treatment, while cytokine production was increased. In CLL cells, we observed a downregulation of immunosuppression, adhesion, and migration proteins. Adaptation at molecular level, characterized by an increase in cancer cell fraction of CLL cells with mutated driver genes, was observed in around half of the patients and was associated with retained migrative capacity towards CXCL12/CXCR4 axis. Interestingly, BTK C481S mutations were detected as early as after 6 months of treatment, particularly enriched in subsets of malignant cells retaining migrative capacity. These CLL cells with potential migrative capacity under ibrutinib also exhibited a distinct transcriptomic profile including upregulation of mTOR-AKT and MYC pathways. We identified the high expression of TMBIM6 as a potential novel independent poor prognostic factor. Of note, BIA, a TMBIM6 antagonist, induced CLL cell apoptosis and synergized with ibrutinib. In summary, our comprehensive multi-omics analysis of CLL patients undergoing ibrutinib therapy has unveiled early immunomodulatory effects on T cells and adaptative mechanisms in CLL cells. These findings can contribute to the identification of resistance mechanisms and the discovery of novel therapeutic targets.
依鲁替尼持续治疗不仅能控制慢性淋巴细胞白血病(CLL)患者的肿瘤,还能增强其T细胞功能。我们对接受一线依鲁替尼治疗的CLL患者样本进行了纵向多组学分析,以确定在持续治疗的前12个月中对布鲁顿酪氨酸激酶(BTK)抑制的潜在适应性机制。我们发现,依鲁替尼可导致耗竭标志物表达降低,调节性T细胞和T滤泡辅助细胞的比例恢复至健康供体水平。在功能上,T细胞中与激活、增殖、分化和代谢相关的基因表达下调;体外刺激后,依鲁替尼治疗仅轻微改变增殖能力,而细胞因子产生增加。在CLL细胞中,我们观察到免疫抑制、黏附和迁移蛋白的下调。在大约一半的患者中观察到分子水平的适应性变化,其特征是具有驱动基因突变的CLL细胞的癌细胞比例增加,并与对CXCL12/CXCR4轴的迁移能力保留相关。有趣的是,早在治疗6个月后就检测到BTK C481S突变,尤其在保留迁移能力的恶性细胞亚群中富集。这些在依鲁替尼作用下具有潜在迁移能力的CLL细胞也表现出独特的转录组谱,包括mTOR-AKT和MYC通路的上调。我们确定TMBIM6的高表达是一种潜在的新型独立不良预后因素。值得注意的是,TMBIM6拮抗剂BIA可诱导CLL细胞凋亡,并与依鲁替尼协同作用。总之,我们对接受依鲁替尼治疗的CLL患者进行的全面多组学分析揭示了对T细胞的早期免疫调节作用以及CLL细胞中的适应性机制。这些发现有助于识别耐药机制和发现新的治疗靶点。