Lipa Alexandra Julia, Andreikovits Patrick, Stoeckl Marco, Domanovits Hans, Schoergenhofer Christian, Schwameis Michael, Grafeneder Juergen
Department of Emergency Medicine, Medical University of Vienna, 1090 Vienna, Austria.
Department of Clinical Pharmacology, Medical University of Vienna, 1090 Vienna, Austria.
J Clin Med. 2025 Mar 1;14(5):1669. doi: 10.3390/jcm14051669.
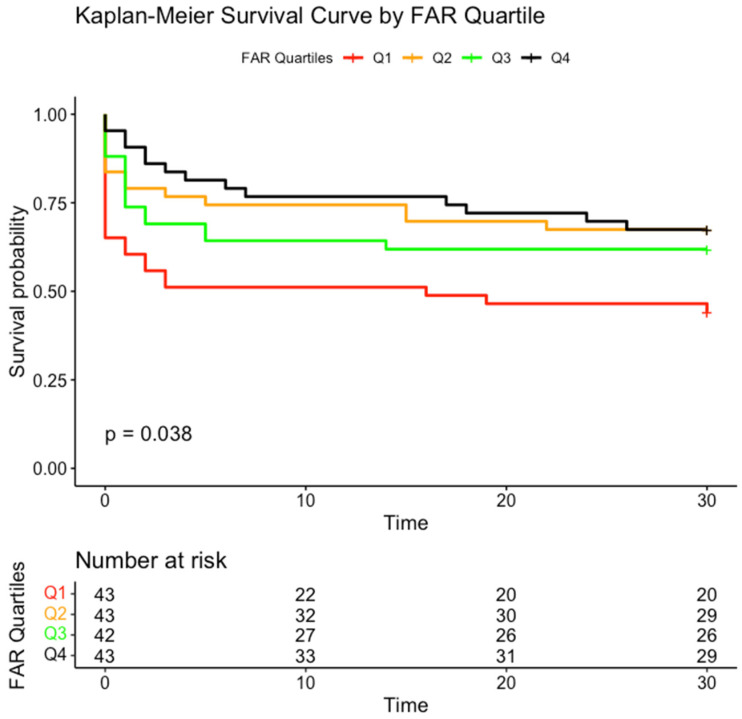
Acute aortic syndrome (AAS) is a life-threatening condition characterized by a high mortality, yet reliable prognostic biomarkers are still lacking. The fibrinogen-to-albumin ratio (FAR) has recently gained attention in cardiovascular research but has not been explored in the context of AAS. This study assessed the association between the FAR and 30-day mortality in AAS patients who presented to the emergency department. We included all AAS patients aged 18 years and older who presented to the emergency department between 2013 and 2021. The outcome measured was 30-day all-cause mortality. Cox regression analysis assessed the relationship between the FAR and the outcome. A total of 171 patients (mean age 67, SD 13.7; 33% female) were included, with 68 (40%) dying within 30 days of admission. Non-survivors had a significantly lower FAR (mean 8.9, SD 4.97) than survivors (mean 10.8, SD 5.44, = 0.02). FAR was significantly associated with 30-day mortality (crude HR 0.935, 95% CI 0.88-0.99, = 0.02). This association remained significant after adjusting for age, sex, cardiopulmonary resuscitation, catecholamine administration, bleeding on admission, and type of AAS (adjusted HR 0.92, 95% CI 0.87-0.98, = 0.01). FAR was independently associated with 30-day mortality in AAS patients who presented to the emergency department. Given its simplicity and cost-effectiveness, it could be a valuable biomarker, especially in resource-limited settings, to improve risk assessment and optimize resource allocation in AAS.
急性主动脉综合征(AAS)是一种危及生命的疾病,死亡率很高,但仍缺乏可靠的预后生物标志物。纤维蛋白原与白蛋白比值(FAR)最近在心血管研究中受到关注,但尚未在AAS背景下进行探讨。本研究评估了急诊科就诊的AAS患者中FAR与30天死亡率之间的关联。我们纳入了2013年至2021年间在急诊科就诊的所有18岁及以上的AAS患者。测量的结局是30天全因死亡率。Cox回归分析评估了FAR与结局之间的关系。共纳入171例患者(平均年龄67岁,标准差13.7;33%为女性),其中68例(40%)在入院后30天内死亡。非幸存者的FAR(平均8.9,标准差4.97)显著低于幸存者(平均10.8,标准差5.44,P = 0.02)。FAR与30天死亡率显著相关(粗风险比0.935,95%置信区间0.88 - 0.99,P = 0.02)。在调整年龄、性别、心肺复苏、儿茶酚胺使用、入院时出血和AAS类型后,这种关联仍然显著(调整后风险比0.92,95%置信区间0.87 - 0.98,P = 0.01)。FAR与急诊科就诊的AAS患者的30天死亡率独立相关。鉴于其简单性和成本效益,它可能是一种有价值的生物标志物,特别是在资源有限的环境中,可用于改善AAS的风险评估和优化资源分配。