He Yunsen, Huang Qinjiang, Bao Mingbin, Zhang Mengjun, Hou Xiaolin, Liu Ping, Tao Ye, Li Hongliang, Li Kun, Liu Li, Guo Lili, Wang Hao, Zhang Zhou, Wu Bo
Department of Neurosurgery, Sichuan Lansheng Brain Hospital and Shanghai Lansheng Brain Hospital Investment Co., Ltd., Chengdu, 610036, Sichuan, People's Republic of China.
Department of Neurosurgery, Chengdu wenjiang District people's hospital, Chengdu, 611130, Sichuan, People's Republic of China.
Sci Rep. 2025 Mar 17;15(1):9197. doi: 10.1038/s41598-025-86528-4.
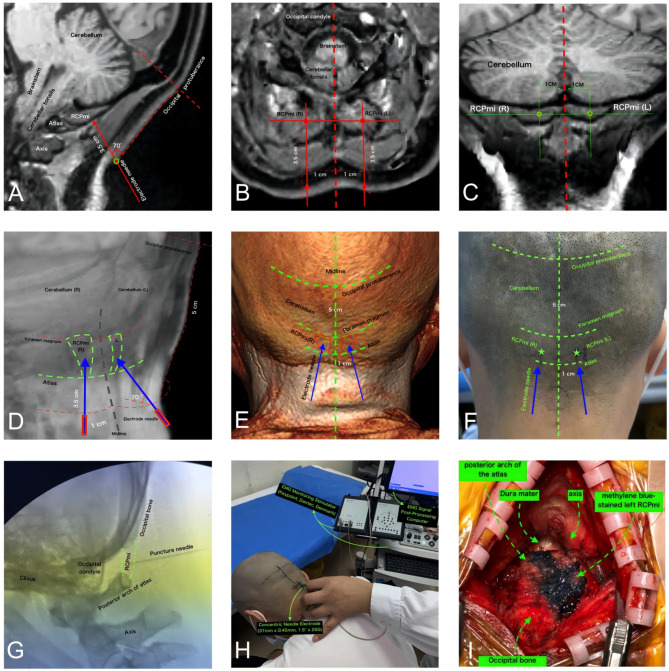
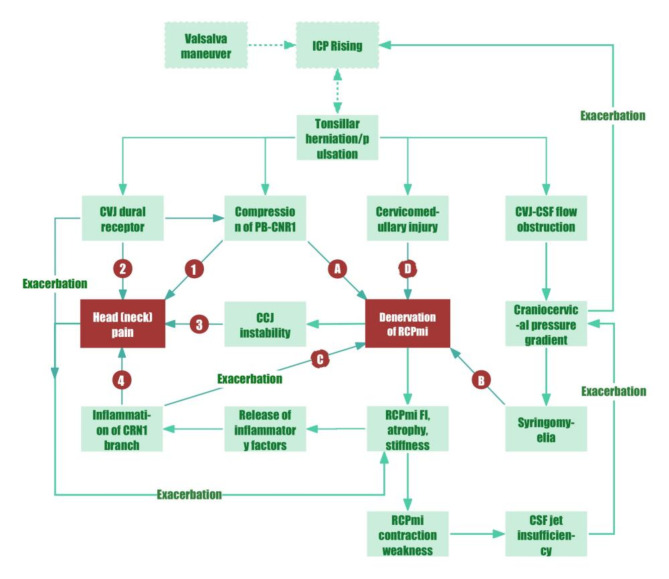
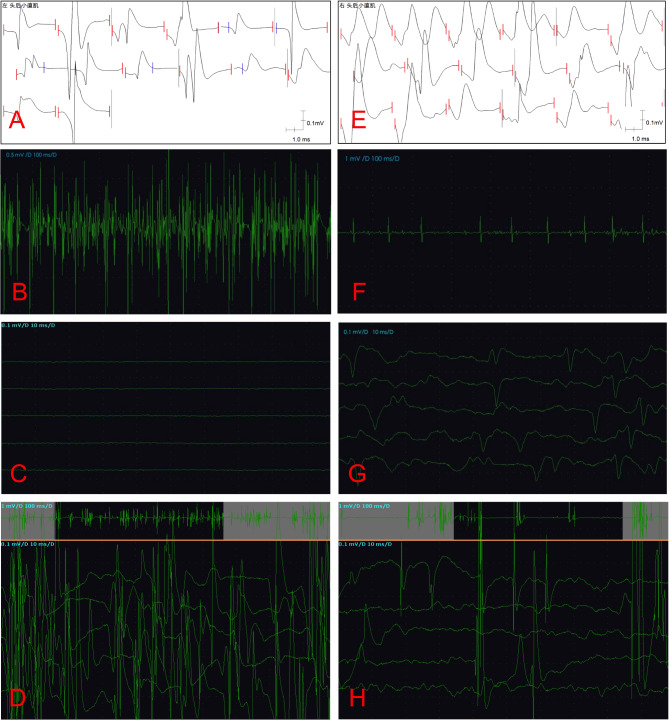
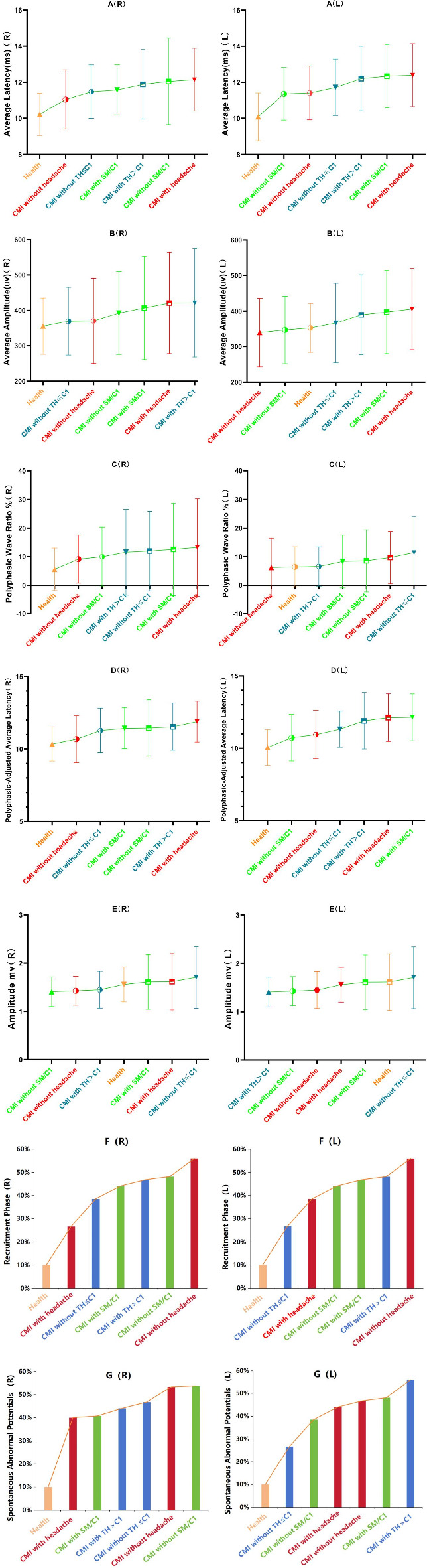
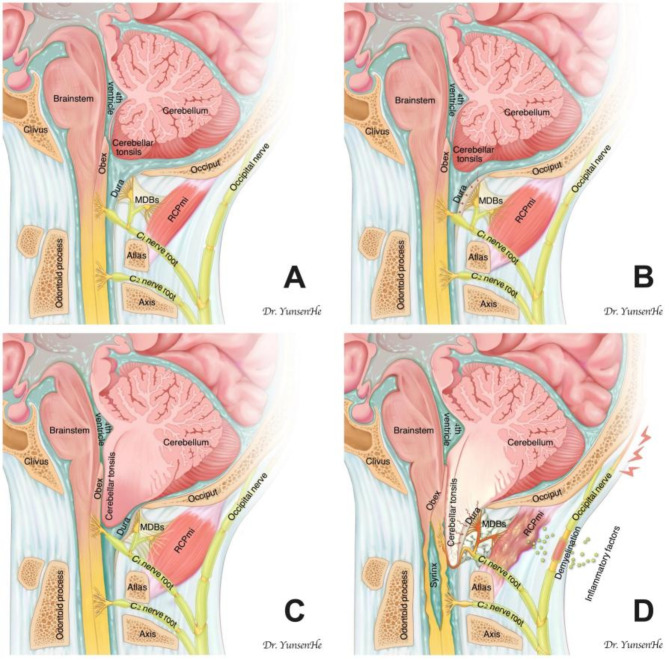
Chiari malformation type I (CMI) typically manifests with Valsalva-induced occipital headaches and commonly co-occurs with syringomyelia. The disruption of cerebrospinal fluid (CSF) dynamics at the craniocervical junction (CCJ) is a key pathophysiological feature. The rectus capitis posterior minor (RCPmi), innervated by the C1 nerve root's posterior branch, significantly facilitates CSF flow at the CCJ, correlating closely with occipital headaches. This study aims to explore RCPmi functionality in CMI patients compared to healthy controls using needle electromyography (nEMG). Data from adult CMI patients and a health group collected from January 2023 to May 2024 were analyzed. Both groups underwent bilateral RCPmi nEMG testing, assessing mean duration, amplitude, multiphasic wave ratio, recruitment phase amplitude, and spontaneous potentials during Valsalva maneuvers. We conducted a double-blinded evaluation, with additional subgroup analyses based on headache presence, tonsillar herniation relative to the C1 vertebra, and syringomyelia involvement. The study included 40 CMI patients and 30 healthy controls with no demographic differences. Healthy controls displayed stable RCPmi-nEMG parameters, with intense electrical activity during Valsalva maneuvers. In contrast, CMI patients exhibited substantial denervation damage in bilateral RCPmi, particularly during Valsalva maneuvers, characterized by insufficient electrical signal response and sparse motor units. Subgroup analysis revealed increased denervation in patients with headaches, extensive tonsillar herniation, and syringomyelia involving C1. RCPmi plays a critical role in maintaining cranio-cervical stability and modulating intracranial pressure, especially during Valsalva maneuvers. Compared to controls, CMI patients show widespread denervation damage in RCPmi, strongly linked to enhanced obstruction of CCJ-CSF flow and typical headache symptoms. This denervation damage, likely related to pathological factors like C1 nerve root compression by herniated cerebellar tonsils and inflammatory mediator release at the CCJ, highlights the functional failure of RCPmi as a novel target for understanding the headache mechanism in CMI and for developing pain interventions.
I型Chiari畸形(CMI)通常表现为瓦尔萨尔瓦动作诱发的枕部头痛,且常与脊髓空洞症同时出现。颅颈交界区(CCJ)脑脊液(CSF)动力学的破坏是关键的病理生理特征。由C1神经根后支支配的头后小直肌(RCPmi)显著促进CCJ处的脑脊液流动,与枕部头痛密切相关。本研究旨在通过针极肌电图(nEMG)探讨CMI患者与健康对照相比RCPmi的功能。分析了2023年1月至2024年5月收集的成年CMI患者和健康组的数据。两组均接受双侧RCPmi的nEMG测试,评估瓦尔萨尔瓦动作期间的平均持续时间、波幅、多相波比率、募集期波幅和自发电位。我们进行了双盲评估,并根据头痛的存在、扁桃体相对于C1椎体的疝出以及脊髓空洞症的累及情况进行了额外的亚组分析。该研究纳入了40例CMI患者和30例健康对照,两组在人口统计学上无差异。健康对照的RCPmi-nEMG参数稳定,在瓦尔萨尔瓦动作期间有强烈的电活动。相比之下,CMI患者双侧RCPmi出现大量去神经损伤,尤其是在瓦尔萨尔瓦动作期间,其特征为电信号反应不足和运动单位稀疏。亚组分析显示,头痛患者、广泛扁桃体疝出患者以及累及C1的脊髓空洞症患者的去神经情况增加。RCPmi在维持颅颈稳定性和调节颅内压方面起着关键作用,尤其是在瓦尔萨尔瓦动作期间。与对照组相比,CMI患者的RCPmi出现广泛的去神经损伤,这与CCJ-CSF流动的阻塞增强和典型头痛症状密切相关。这种去神经损伤可能与诸如小脑扁桃体疝压迫C1神经根以及CCJ处炎症介质释放等病理因素有关,突出了RCPmi的功能障碍,这是理解CMI头痛机制和开发疼痛干预措施的一个新靶点。