Jaan Ali, Sarfraz Zouina, Maryyum Adeena, Farooq Umer, Ashraf Muhammad Farhan, Warraich Fatima, Mcfarland Mark S, Gutman Jason, Dunnigan Karin
Department of Internal Medicine, Rochester General Hospital, Rochester, NY, USA.
Department of Medicine, Fatima Jinnah Medical University, Queen's Road, Mozang Chungi, Lahore, 54000, Pakistan.
BMC Gastroenterol. 2025 Mar 18;25(1):183. doi: 10.1186/s12876-025-03755-9.
This study investigates the role of interhospital transfer (IHT) in lower gastrointestinal bleeding (LGIB) management and its impact on patient outcomes, focusing on mortality rates, complication occurrences, procedural performance, and resource utilization in patients diagnosed with LGIB.
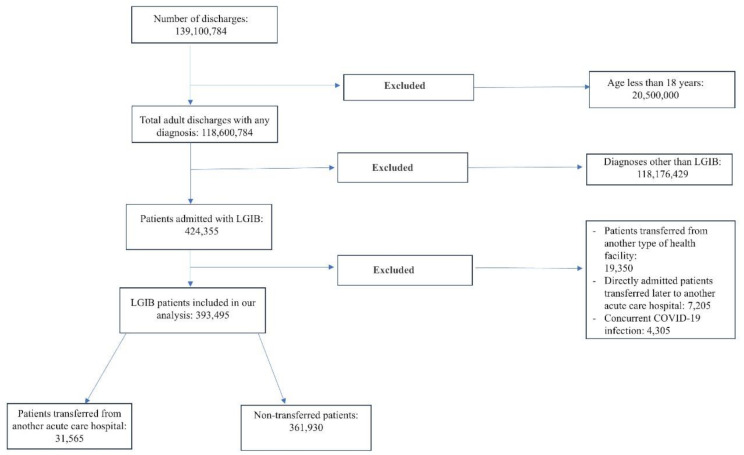
This retrospective cohort study used data from the National Inpatient Sample database from 2017 to 2020. It included adult patients diagnosed with LGIB, assessing the impact of IHT on outcomes such as mortality, complication rates, procedural performance, and resource utilization. Adjusted odds ratios (AOR) and adjusted mean differences (AMD) were used to evaluate these impacts.
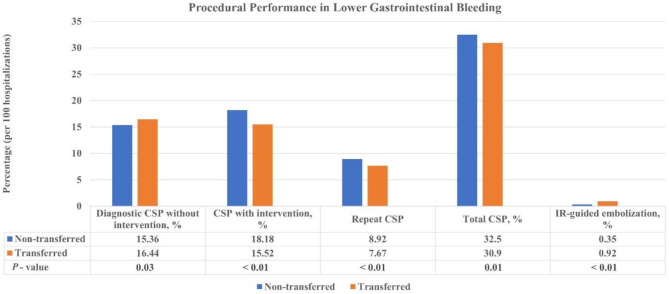
A total of 393,495 LGIB patients were analyzed, with 31,565 (8.02%) undergoing interhospital transfer. Transferred patients exhibited significantly higher inpatient mortality (AOR 1.96, P < 0.01). They also faced increased risks of acute kidney injury (AOR 1.32, P < 0.01), septic shock (AOR 2.11, P < 0.01), and intensive care unit admission (AOR: 2.61, P < 0.01). These patients were more likely to undergo interventional radiology-guided embolization (AOR 2.68, P < 0.01) and showed variations in colonoscopy procedures. Resource utilization was also higher among transferred patients, with an increased mean length of hospital stay by 4.37 days (P < 0.01) and higher hospitalization charges (mean difference $61,239, P < 0.01).
Interhospital transfer in LGIB patients is associated with increased mortality, greater resource utilization, and the need for more specialized procedural interventions. Enhanced clinical vigilance and tailored resource allocation for transferred LGIB patients are necessary. Future research should optimize care strategies for these high-risk patients.
本研究调查了院间转运(IHT)在低位胃肠道出血(LGIB)管理中的作用及其对患者结局的影响,重点关注确诊为LGIB患者的死亡率、并发症发生率、手术操作情况及资源利用情况。
这项回顾性队列研究使用了2017年至2020年国家住院样本数据库中的数据。研究纳入了确诊为LGIB的成年患者,评估院间转运对死亡率、并发症发生率、手术操作情况及资源利用等结局的影响。采用调整后的优势比(AOR)和调整后的均值差(AMD)来评估这些影响。
共分析了393,495例LGIB患者,其中31,565例(8.02%)接受了院间转运。转运患者的住院死亡率显著更高(AOR 1.96,P < 0.01)。他们还面临急性肾损伤(AOR 1.32,P < 0.01)、感染性休克(AOR 2.11,P < 0.01)及入住重症监护病房(AOR:2.61,P < 0.01)风险增加的情况。这些患者更有可能接受介入放射学引导下的栓塞治疗(AOR 2.68,P < 0.01),且结肠镜检查操作存在差异。转运患者的资源利用也更高,平均住院时间增加了4.37天(P < 0.01),住院费用更高(均值差61,239美元,P < 0.01)。
LGIB患者的院间转运与死亡率增加、资源利用增加以及需要更专业的手术干预相关。有必要加强对转运LGIB患者的临床监测并进行针对性的资源分配。未来的研究应优化这些高危患者的护理策略。