Abate Biruk Beletew, Sendekie Ashenafi Kibret, Alamaw Addis Wondimagegn, Tegegne Kindie Mekuria, Kitaw Tegene Atamenta, Bizuayehu Molla Azmeraw, Kassaw Amare, Yilak Gizachew, Zemariam Alemu Birara, Tilahun Befkad Derese
School of Population Health, Curtin University, Perth, Australia (Abate).
College of Medicine and Health Sciences, Woldia University, Woldia, Ethiopia (Abate).
AJOG Glob Rep. 2025 Jan 20;5(1):100441. doi: 10.1016/j.xagr.2025.100441. eCollection 2025 Feb.
This study aimed to assess the magnitude, determinants, and outcomes of adolescent pregnancy by combining data from previous systematic reviews and meta-analyses.
Online databases.
Systematic Review and Meta-analysis.
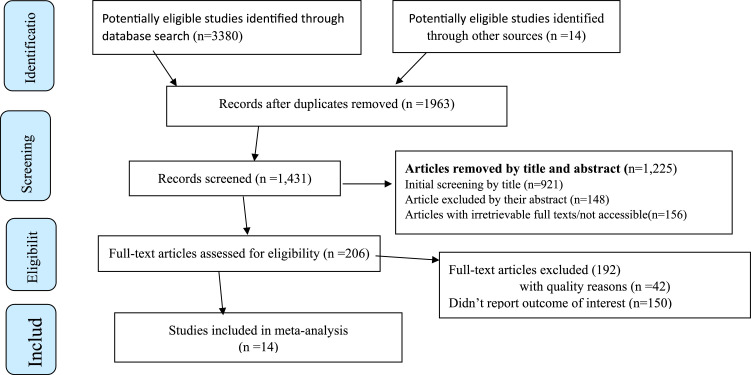
Using the Preferred Reporting Items for Systematic Reviews and Meta-Analyses guidelines, PubMed, Embase, Scopus, Web of Sciences, Cochrane Database of Systematic Reviews, Scopus, and Google Scholar, which reported the magnitude, predictors, and/or outcomes of adolescent pregnancy, were searched. The quality of the included studies was assessed using the Assessment of Multiple Systematic Reviews. A weighted inverse variance random-effects model was used to determine the pooled estimates. In addition, subgroup heterogeneity, publication bias, and sensitivity were assessed.
A total of 14 systematic reviews and meta-analyses involving 677,431 participants were included in the final analysis of this umbrella review. The pooled prevalence of adolescent pregnancy from global systematic reviews and meta-analyses was found to be 17.90 (95% confidence interval, 12.25-23.54). Level of education (adjusted odds ratio ranging from 1.40 to 9.07), socioeconomic status (lower: adjusted odds ratio ranging from 1.13 to 3.81), residency (rural: adjusted odds ratio ranging from 1.80 to 3.60), abuse (adjusted odds ratio ranging from 2.21 to 3.83), marital status (married: adjusted odds ratio ranging from 1.27 to 6.02), and contraceptive use (no: adjusted odds ratio ranging from 0.19 to 3.53) were identified as predictors of adolescent pregnancy. Anemia (adjusted odds ratio, 1.49; 95% confidence interval, 0.29-1.69; = 91.7%), stillbirth (adjusted odds ratio, 1.71; 95% confidence interval, 0.24-3.17; = 61.3%), preeclampsia/eclampsia, (adjusted odds ratio, 1.63; 95% confidence interval, 0.72-2.55), preterm birth (adjusted odds ratio, 1.90; 95% confidence interval, 1.36-2.40), and low birthweight (adjusted odds ratio, 1.46; 95% confidence interval, 1.25-1.66) were found to be significant complications of adolescent pregnancy in a global context.
The prevalence of adolescent pregnancy varied significantly across previous systematic reviews and meta-analyses. The key determinants identified included low socioeconomic status, rural residency, a history of abuse, early marriage, and no contraceptive use. The complications associated with adolescent pregnancy included anemia, stillbirth, preeclampsia/eclampsia, preterm birth, and low birthweight. To reduce the burden of adolescent pregnancy, collaborative efforts are required from global, regional, and local stakeholders, such as policymakers and reproductive health program planners, through health education and training that focus on the most vulnerable populations.
本研究旨在通过整合以往系统评价和荟萃分析的数据,评估青少年怀孕的规模、决定因素和后果。
在线数据库。
系统评价和荟萃分析。
按照系统评价和荟萃分析的首选报告项目指南,检索了PubMed、Embase、Scopus、科学网、Cochrane系统评价数据库、Scopus和谷歌学术,这些数据库报告了青少年怀孕的规模、预测因素和/或后果。使用多重系统评价评估法对纳入研究的质量进行评估。采用加权逆方差随机效应模型来确定合并估计值。此外,还评估了亚组异质性、发表偏倚和敏感性。
本伞状评价的最终分析共纳入了14项系统评价和荟萃分析,涉及677431名参与者。全球系统评价和荟萃分析得出的青少年怀孕合并患病率为17.90(95%置信区间,12.25 - 23.54)。教育程度(调整优势比范围为1.40至9.07)、社会经济地位(较低:调整优势比范围为1.13至3.81)、居住地区(农村:调整优势比范围为1.80至3.60)、虐待史(调整优势比范围为2.21至3.83)、婚姻状况(已婚:调整优势比范围为1.27至6.02)以及避孕措施使用情况(未使用:调整优势比范围为0.19至3.53)被确定为青少年怀孕的预测因素。在全球范围内,贫血(调整优势比,1.49;95%置信区间,0.29 - 1.69;I² = 91.7%)、死产(调整优势比,1.71;95%置信区间,0.24 - 3.17;I² = 61.3%)、先兆子痫/子痫(调整优势比,1.63;95%置信区间,0.72 - 2.55)、早产(调整优势比,1.90;95%置信区间,1.36 - 2.40)和低出生体重(调整优势比,1.46;95%置信区间,1.25 - 1.66)被发现是青少年怀孕的显著并发症。
以往系统评价和荟萃分析中青少年怀孕的患病率差异显著。确定的关键决定因素包括社会经济地位低、农村居住、虐待史、早婚以及未使用避孕措施。与青少年怀孕相关的并发症包括贫血、死产、先兆子痫/子痫、早产和低出生体重。为减轻青少年怀孕的负担,全球、区域和地方的利益相关者,如政策制定者和生殖健康项目规划者,需要通过针对最脆弱人群的健康教育和培训共同努力。