Dirven Linda, Machingura Abigirl, van den Bent Martin J, Coens Corneel, Bottomley Andrew, Brandes Alba A, Domont Julien, Idbaih Ahmed, Koekkoek Johan A F, Reijneveld Jaap C, Platten Michael, Wick Wolfgang, Taphoorn Martin J B
Department of Neurology, Haaglanden Medical Center, The Hague, The Netherlands.
Department of Neurology, Leiden University Medical Center, Leiden, The Netherlands.
Neurooncol Pract. 2024 Sep 25;12(2):209-218. doi: 10.1093/nop/npae091. eCollection 2025 Apr.
Progression-free survival, but not overall survival, was prolonged with bevacizumab and lomustine compared to lomustine only in the randomized phase 3 European Organization for Research and Treatment of Cancer (EORTC) 26101 study.
To evaluate the impact of treatment on health-related quality of life (HRQoL) in progressive glioblastoma patients participating in the EORTC 26101 study.
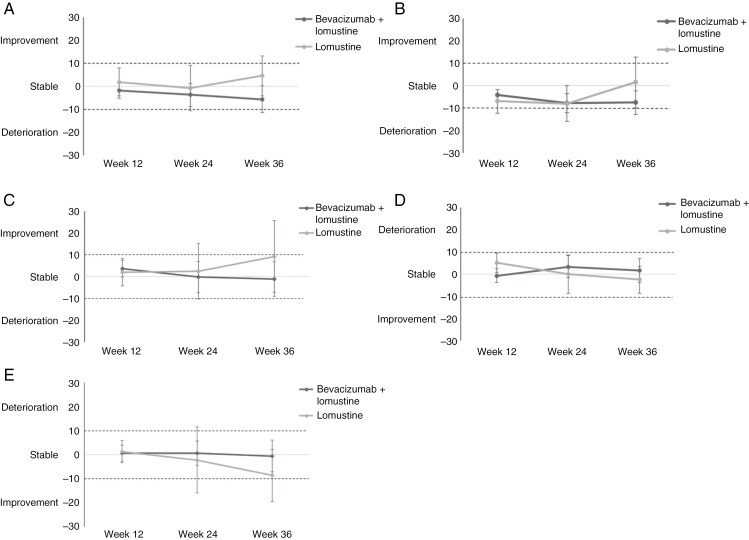
Patients with progressive glioblastoma, after standard radio-chemotherapy, were 2:1 randomized to either BEV/LOM or LOM. HRQoL was a secondary trial outcome and assessed using the EORTC QLQ-C30 and QLQ-BN20 questionnaires at baseline, and subsequently every 12 weeks. Predefined scales for analysis were global health status (GH), physical functioning, social functioning (SF), motor dysfunction, and communication deficit. The primary endpoint was HRQoL during the last assessment up to week 36. Moreover, time to HRQoL deterioration (TTD) and HRQoL deterioration-free survival (DFS) were calculated.
Out of 437 patients, 402 (92%) patients had a baseline HRQoL assessment, which dropped to 66% at week 36. During the last assessment up to week 36, no differences were observed for predefined scales, apart from SF being clinically relevant lower in the combination arm (mean 66.0 versus 81.0, = .001). Of note, the baseline SF score was 66.4 for patients in the combination arm, showing stable SF. Median DFS was significantly longer in the combination arm (12.4 weeks) compared to lomustine alone (6.7 weeks), reflecting the difference in time to progression between arms. TTD, not including progression as an event, was not different between treatment arms (median 13.0 versus 12.9 weeks).
The addition of bevacizumab to lomustine did not negatively affect HRQoL during the progression-free period.
在随机3期欧洲癌症研究与治疗组织(EORTC)26101研究中,与仅使用洛莫司汀相比,贝伐单抗联合洛莫司汀可延长无进展生存期,但不能延长总生存期。
评估治疗对参与EORTC 26101研究的进展性胶质母细胞瘤患者健康相关生活质量(HRQoL)的影响。
标准放化疗后进展性胶质母细胞瘤患者按2:1随机分为BEV/LOM组或LOM组。HRQoL是次要试验结局,在基线时使用EORTC QLQ-C30和QLQ-BN20问卷进行评估,随后每12周评估一次。用于分析的预定义量表包括总体健康状况(GH)、身体功能、社会功能(SF)、运动功能障碍和沟通障碍。主要终点是第36周最后一次评估时的HRQoL。此外,计算了HRQoL恶化时间(TTD)和无HRQoL恶化生存期(DFS)。
437例患者中,402例(92%)患者进行了基线HRQoL评估,在第36周时降至66%。在第36周最后一次评估时,除联合治疗组的SF在临床上显著较低(均值66.0对81.0,P = 0.001)外,预定义量表未观察到差异。值得注意的是,联合治疗组患者的基线SF评分为66.4,显示SF稳定。联合治疗组的中位DFS(12.4周)明显长于单独使用洛莫司汀组(6.7周),这反映了两组之间疾病进展时间的差异。不将疾病进展作为事件的TTD在治疗组之间没有差异(中位值13.0对12.9周)。
在无进展期,洛莫司汀联合贝伐单抗对HRQoL没有负面影响。