Shinmura Hiroki, Tsunoda Youhei, Matsushima Takashi, Kurashina Ryuhei, Watanabe Asako, Harigane Eika, Ouchi Nozomi, Suzuki Shunji
Department of Obstetrics and Gynecology, Nippon Medical School Musashikosugi Hospital, Kawasaki, Kanagawa, Japan.
Department of Obstetrics and Gynecology, Nippon Medical School Hospital, Bunkyo, Tokyo, Japan.
PLoS Med. 2025 Mar 25;22(3):e1004555. doi: 10.1371/journal.pmed.1004555. eCollection 2025 Mar.
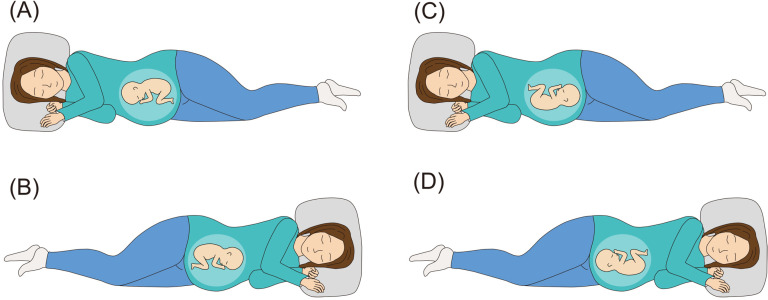
In Japan, the lateral position method is known as a postural therapy for breech presentation wherein the mother lies down in lateral position according to the orientation of the fetal back. Few studies have formally tested lateral position management for breech presentation, and no method exists to prevent breech recurrence after cephalic version. We hypothesized that postural management comprising a combination of opposite-side lateral position for breech presentation and same-side lateral position after cephalic version demonstrates a clinically relevant effect size on breech presentation.
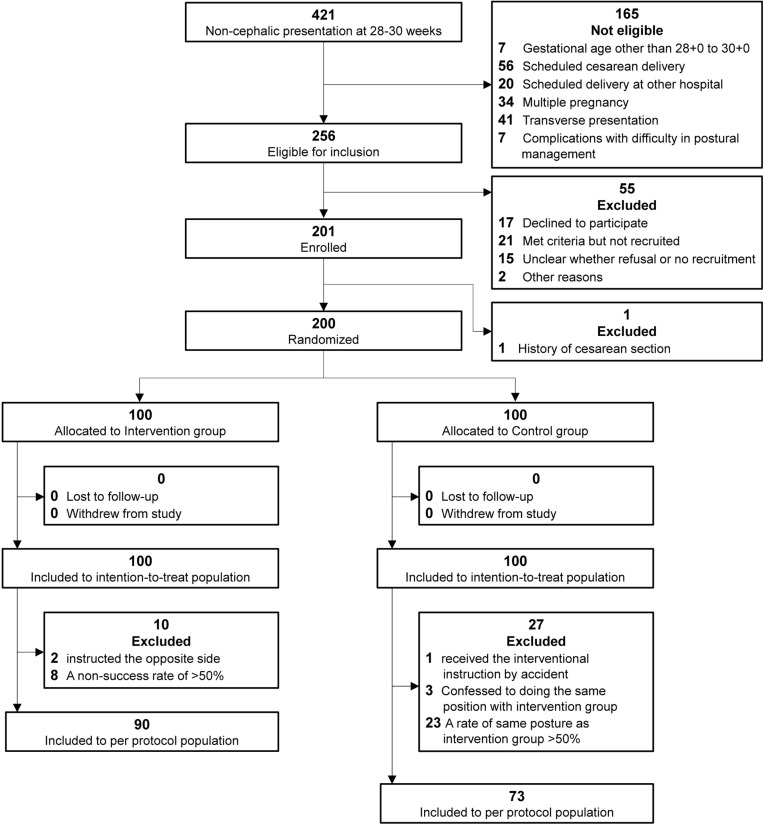
We conducted a stratified, open-label randomized controlled trial at an academic hospital in Kawasaki, Japan. A total of 200 women diagnosed with breech presentation between 28 + 0 and 30 + 0 gestational weeks were randomized to postural management (n = 100) or control (no intervention, n = 100) group. The intervention was instruction every 2 weeks on lying in the lateral position on the opposite-side of fetal back for breech presentation and on the same-side of fetal back for head-first presentation. The primary outcome was the rate of fetuses in breech presentation at 37 weeks of gestation, and the secondary outcomes were cesarean delivery, cesarean delivery for breech presentation, head presentation 2, 4, and 6 weeks later, breech presentation recurrence, and adverse events. Breech presentation rate at 37 gestational weeks was 11% in the intervention group, using the combination of the opposite-side and same-side lateral positions, compared with 19% in the control group. However, we found no statistical significance in the intention-to-treat analysis (11% [11/100] versus 19% [19/100]; relative risk, 0.58 [95% CI, 0.29 to 1.15]; p = 0.11). In the control group, 23 participants (23%) unknowingly took the same posture as the intervention group, and the prespecified per-protocol analysis excluding crossover found the same direction of effect but with statistical significance. In the intention-to-treat analysis, the intervention group had a higher cephalic version rate 2 weeks after the instruction (69% [69/100] versus 54% [54/100]; relative risk, 0.67 [95% CI, 0.47 to 0.96]; p = 0.029), and lower breech presentation recurrence rates (2% [2/91] versus 10% [9/88]; relative risk, 0.22 [95% CI, 0.048 to 0.97]; p = 0.031) than the control group. Regarding adverse events in the intervention group, three participants experienced discomfort and one participant complained of pain in the lateral abdomen; these symptoms resolved spontaneously.
For breech presentation at the beginning of the third trimester, providing postural therapy instruction on opposite-side lateral positioning and same-side lateral positioning was associated with 8% reduction of breech fetuses at 37 gestational weeks compared with the control group, but this primary endpoint did not reach statistical significance. Regarding the secondary endpoints, the intervention group showed a significantly higher rate of cephalic version after 2 weeks and lower rate of breech recurrence. The direction of the effect of postural therapy based on fetal back position on breech presentation was promising, and further research to validate this approach, with consideration for unplanned participant crossover, may be warranted.
UMIN Clinical Trials Registry (UMIN000043613, https://center6.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000049800).
在日本,侧卧位法是一种用于臀位的体位疗法,即母亲根据胎儿背部的朝向采取侧卧位。很少有研究对臀位的侧卧位管理进行正式测试,并且不存在预防头位转位后臀位复发的方法。我们假设,由臀位时的对侧侧卧位和头位转位后的同侧侧卧位组合而成的体位管理对臀位具有临床相关的效应量。
我们在日本川崎的一家学术医院进行了一项分层、开放标签的随机对照试验。共有200名在孕28 + 0至30 + 0周被诊断为臀位的女性被随机分为体位管理组(n = 100)或对照组(不干预,n = 100)。干预措施是每2周指导一次,臀位时躺在胎儿背部对侧的侧卧位,头先露时躺在胎儿背部同侧的侧卧位。主要结局是妊娠37周时臀位胎儿的比例,次要结局包括剖宫产、因臀位行剖宫产、2周、4周和6周后头先露、臀位复发以及不良事件。干预组采用对侧和同侧侧卧位组合,妊娠37周时臀位率为11%,而对照组为19%。然而,在意向性分析中我们未发现统计学意义(11% [11/100] 对19% [19/100];相对风险,0.58 [95% CI,0.29至1.15];p = 0.11)。在对照组中,23名参与者(23%)在不知情的情况下采取了与干预组相同的体位,排除交叉情况的预先指定的符合方案分析发现了相同的效应方向,但具有统计学意义。在意向性分析中,干预组在指导后2周的头位转位率更高(69% [69/100] 对54% [54/当与对照组相比,干预组的臀位复发率更低(2% [2/91] 对10% [9/88];相对风险,0.22 [95% CI,0.048至0.97];p = 0.03)。关于干预组的不良事件,3名参与者感到不适,1名参与者抱怨侧腹疼痛;这些症状自行缓解。
对于孕晚期开始时的臀位,提供对侧侧卧位和同侧侧卧位的体位疗法指导与对照组相比,妊娠37周时臀位胎儿减少了8%,但这一主要终点未达到统计学意义。关于次要终点,干预组在2周后显示出头位转位率显著更高,臀位复发率更低。基于胎儿背部位置的体位疗法对臀位的效应方向是有前景的,可能需要进一步研究以验证这种方法,同时考虑计划外的参与者交叉情况。
UMIN临床试验注册中心(UMIN000043613,https://center6.umin.ac.jp/cgi-open-bin/ctr_e/ctr_view.cgi?recptno=R000049800)。 100];相对风险,0.67 [95% CI,0.47至0.96];p = 0.029),并且