Allen Brett, Knutson Alexis, Iftekhar Noama, Giles Casey, Patterson Jarrell, MacDavid Joshua, Baynosa Richard
Department of Plastic Surgery, University of Nevada, Las Vegas, NV 89102, USA.
J Clin Med. 2025 Mar 19;14(6):2100. doi: 10.3390/jcm14062100.
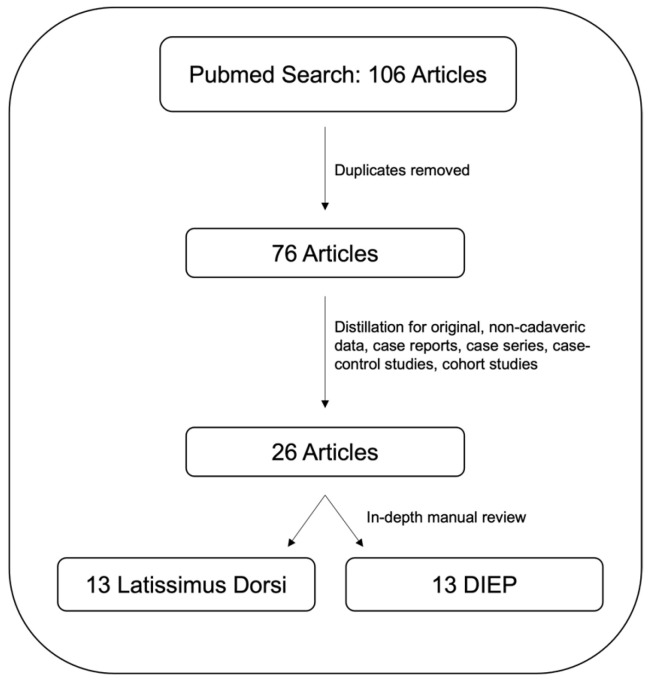
Breast cancer is the second most common cancer in women with an improving mortality rate and a growing need for reconstruction following oncologic resection. Advancements in robotic surgery and minimally invasive techniques have offered refinement to traditional open techniques of flap harvest for reconstruction, particularly regarding improved donor site morbidity. The literature review was based on a PubMed database search using the keyword "Robotic breast reconstruction" in conjunction with the Boolean operators "Flap", "Latissimus", and "DIEP" to specify the search. In total, 106 results were generated, which were then manually reviewed and condensed for a comprehensive stance on the current status, technique, variations, and outcomes for robotic breast reconstruction. Robotic technique has been described for the latissimus dorsi (LD) and deep inferior epigastric perforator (DIEP) flaps for breast reconstruction. For LD, robotic flap harvest reduces donor site morbidity, incisional length, and hospital length of stay, with similar complication rates for seroma/hematoma/infection, and longer operative times. Robotic LD procedures have been described in conjunction with single-site nipple-sparing mastectomy and flap elevation leading to a full minimally invasive resection and reconstruction from one lateral incision. Robotic DIEP harvest offers a considerably smaller fascial incision/rectus muscle dissection and has a comparable complication rate to traditional techniques with shorter hospital length of stay, and improved pain, at the expense of longer operating times. Data on hernia/bulge reduction from robotic techniques is limited and not yet available. Robotic breast reconstruction offers great potential for improving breast reconstruction in terms of donor site morbidity, length of incision, hospital length of stay at the cost of longer operating times, and increased technical skill/specialization, but it has yet to be proven on a large scale with long-term outcome data. Multi-center, prospective clinical data and trials are needed to help elucidate the potential for equivalence and superiority of the minimally invasive approach compared to standard open techniques, but the future is promising for robotic surgery in breast cancer and breast reconstruction.
乳腺癌是女性中第二常见的癌症,其死亡率在不断改善,肿瘤切除术后乳房重建的需求也日益增加。机器人手术和微创技术的进步为传统的皮瓣切取开放技术用于乳房重建带来了改进,特别是在改善供区发病率方面。文献综述基于在PubMed数据库中使用关键词“机器人乳房重建”并结合布尔运算符“皮瓣”“背阔肌”和“腹壁下深动脉穿支”进行搜索。总共产生了106条结果,然后对其进行人工审查和汇总,以全面了解机器人乳房重建的现状、技术、变体和结果。机器人技术已被描述用于背阔肌(LD)和腹壁下深动脉穿支(DIEP)皮瓣进行乳房重建。对于LD皮瓣,机器人皮瓣切取可降低供区发病率、切口长度和住院时间,血清肿/血肿/感染的并发症发生率相似,但手术时间更长。机器人LD手术已与单部位保乳乳房切除术和皮瓣提升术相结合进行描述,可从一个外侧切口实现完全微创切除和重建。机器人DIEP切取提供了小得多的筋膜切口/腹直肌分离,并发症发生率与传统技术相当,住院时间更短,疼痛改善,但手术时间更长。关于机器人技术减少疝气/隆起的数据有限且尚未可得。机器人乳房重建在改善乳房重建方面具有巨大潜力,可降低供区发病率、切口长度和住院时间,但代价是手术时间延长以及技术技能/专业化程度提高,不过尚未通过大规模长期结果数据得到证实。需要多中心、前瞻性临床数据和试验来帮助阐明微创方法与标准开放技术相比的等效性和优越性潜力,但机器人手术在乳腺癌和乳房重建方面的前景广阔。