Mohammed Huda, Gabra Ingie M, Halawa Nouran, Naeem Saira, Ogah Cyprian O, Nath Tuheen Sankar
Colorectal Surgery, Luton and Dunstable Hospital, Luton, GBR.
Anesthesiology, John Muir Health, Walnut Creek Medical Center, Walnut Creek, USA.
Cureus. 2024 Nov 2;16(11):e72877. doi: 10.7759/cureus.72877. eCollection 2024 Nov.
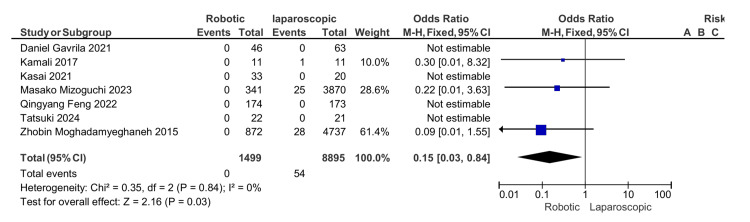
Minimally invasive surgery, especially robotic surgery, has become increasingly popular in colorectal surgery over the last decade. Robotic-assisted surgery has shown better outcomes than conventional laparoscopic surgery because of superior ergonomics, high-resolution three-dimensional cameras, and articulating instruments; however, issues like the long operative time and cost-effectiveness remain unresolved. This study compares the robotic and laparoscopic approach of abdominoperineal resection (APR) for low rectal cancer to evaluate the superiority of robotic surgery in short-term and oncological outcomes. This meta-analysis used Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) guidelines and principles. We conducted a systematic search in the PubMed, Cochrane, Google Scholar, and ResearchGate databases, and seven studies were included after the standardized quality check. Inclusion criteria involved any patient at the age of 18 or above with low rectal cancer who underwent APR with the exclusion of studies that are not in English, patients who underwent open surgery, and patients with recurrent cancer. A total number of 10,331 participants from seven eligible studies were involved in this review and meta-analysis with 1499 in the robotic group and 8,895 in the laparoscopic group. The oncological outcome showed that the positive resection margin is significantly higher in the laparoscopic group with a mean difference (MD) of 0.35, 95% CI (0.14, 0.89), and P = 0.03. The difference in the number of harvested lymph nodes between the robotic and laparoscopic APR is not statistically significant with an OR of 0, 95% CI (-0.19, 0.19), and P = 0.98. The operative time was found to be higher in the robotic group with an MD of 11.25, 95% CI (9.25, 13.04), and P = 0.0001. A higher conversion rate was reported in the laparoscopic group with OR 0.38, 95% CI (0.28, 0.51), and P = 0.00001. The length of the hospital stay was less in the robotic group with an MD of 2, 95% CI (-2.08, -1.92), and P = 0.00001. A lower rate of postoperative ileus was found in the robotic group with an odd ratio of 0.74, 95% CI (0.61,0.89), and P = 0.001, which is statistically significant. The mortality rate and thromboembolic complication also showed a significantly higher rate in the laparoscopic group with an OR of 0.15, 95% CI (0.03, 0.84), and P = 0.03 and an OR of 0.14, 95% CI (0.03, 0.69), and P = 0.02, respectively. There is no statistically significant difference between the robotic and laparoscopic groups in the surgical site infection, urinary dysfunction, cardiac, and pulmonary complications. In conclusion, our study findings indicated that robotic APR has a better short-term outcome and negative circumferential resection margins compared to laparoscopic APR. However, more research and prospective randomized controlled trials are needed to determine the efficiency, cost effectiveness, recurrence, and survival rate in robotic APR.
在过去十年中,微创手术,尤其是机器人手术,在结直肠手术中越来越受欢迎。由于卓越的人体工程学设计、高分辨率三维摄像头和可弯曲器械,机器人辅助手术的效果优于传统腹腔镜手术;然而,手术时间长和成本效益等问题仍未得到解决。本研究比较了低位直肠癌腹会阴联合切除术(APR)的机器人手术和腹腔镜手术方法,以评估机器人手术在短期和肿瘤学结果方面的优势。这项荟萃分析采用了系统评价和荟萃分析的首选报告项目(PRISMA)指南和原则。我们在PubMed、Cochrane、谷歌学术和ResearchGate数据库中进行了系统检索,经过标准化质量检查后纳入了七项研究。纳入标准包括任何年龄在18岁及以上的低位直肠癌患者,这些患者接受了APR手术,排除了非英文研究、接受开放手术的患者以及复发性癌症患者。本综述和荟萃分析共纳入了七项符合条件研究的10331名参与者,其中机器人手术组1499名,腹腔镜手术组8895名。肿瘤学结果显示,腹腔镜手术组的阳性切缘显著更高,平均差(MD)为0.35,95%置信区间(CI)为(0.14,0.89),P = 0.03。机器人辅助APR和腹腔镜APR之间收获淋巴结数量的差异无统计学意义,比值比(OR)为0,95% CI为(-0.19,0.19),P = 0.98。发现机器人手术组的手术时间更长,MD为11.25,95% CI为(9.25,13.04),P = 0.0001。腹腔镜手术组的转化率更高,OR为0.38,95% CI为(0.28,0.51),P = 0.00001。机器人手术组的住院时间更短,MD为2,95% CI为(-2.08,-1.92),P = 0.00001。机器人手术组的术后肠梗阻发生率较低,比值比为0.74,95% CI为(0.61,0.89),P = 0.001,具有统计学意义。腹腔镜手术组的死亡率和血栓栓塞并发症发生率也显著更高,OR分别为0.15,95% CI为(0.03,0.84),P = 0.03和OR为0.14,95% CI为(0.03,0.69),P = 0.02。机器人手术组和腹腔镜手术组在手术部位感染、泌尿系统功能障碍、心脏和肺部并发症方面无统计学显著差异。总之,我们的研究结果表明,与腹腔镜APR相比,机器人APR具有更好的短期结果和阴性环周切缘。然而,需要更多的研究和前瞻性随机对照试验来确定机器人APR的效率、成本效益、复发率和生存率。