Buyukgolcigezli Idil, Tenekeci Ates Kutay, Sahin Ibrahim Halil
Faculty of Medicine, Hacettepe University, Ankara 06230, Turkey.
Department of Biochemistry, Faculty of Medicine, Hacettepe University, Ankara 06230, Turkey.
Cancers (Basel). 2025 Mar 12;17(6):958. doi: 10.3390/cancers17060958.
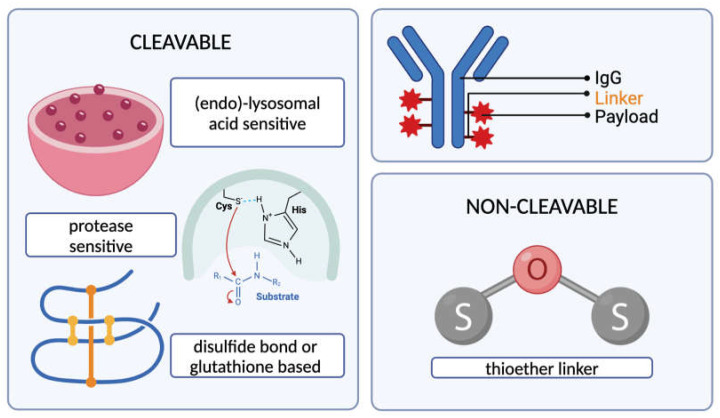
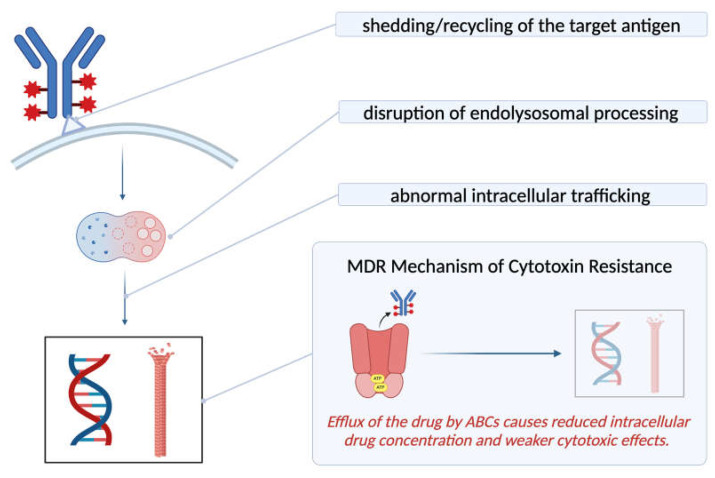
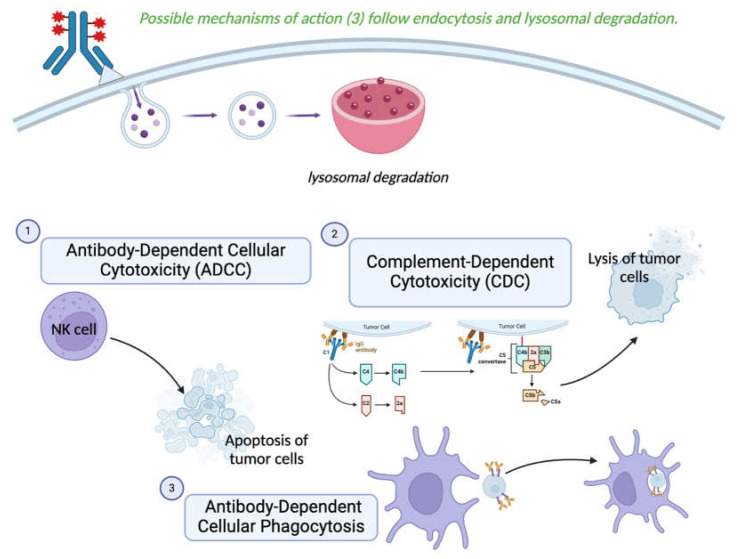
The antibody, linker, and payload moieties all play a significant role in giving the ADC its unique therapeutic potential. The antibody subclass employed in ADCs is determined based on relative individual receptor affinities and pharmacokinetics. Meanwhile, the linker used in an ADC can either be cleavable or non-cleavable. ADC therapy comprises antibody-dependent mechanisms in addition to the direct cytotoxic effects of the payload. These include antibody-dependent cellular cytotoxicity, complement-dependent cytotoxicity, and antibody-dependent cellular phagocytosis, as well as the "bystander effect", which refers to the diffusion of a portion of the cytotoxic molecules out of the target cell, exerting its cytotoxic effect on the adjacent cells. Target antigens of ADCs are expected to be expressed on the membranes of the cancer cells facing the external matrix, although new approaches utilize antigens regarding tumor-associated cells, the tumor microenvironment, or the tumor vasculature. These target antigens of ADCs not only determine the efficacy of these agents but also impact the off-targets and related adverse effects. The majority of ADC-related toxicities are associated with off-targets. The proposed mechanisms of ADC resistance include disrupted intracellular drug trafficking, dysfunctional lysosomal processing, and the efflux of the cytotoxic molecule via ATP-binding cassette (ABC) transporters. The latter mechanism is especially prominent for multi-drug-resistant tumors. An important limitation of ADCs is the penetration of the conjugate into the tumor microenvironment and their delivery to target cancer cells. Cancerous tissues' vascular profile and the steric "binding site barrier" formed around the peripheral vessels of tumors stand as potential challenges of ADC therapy for solid tumors. As research efforts focus on reducing toxicities, overcoming resistance, and improving pharmacokinetics, ADC options for cancer therapy are expected to continue to diversify, including standalone approaches and combination therapies.
抗体、连接子和有效载荷部分在赋予抗体药物偶联物(ADC)独特的治疗潜力方面都发挥着重要作用。ADC中使用的抗体亚类是根据相对个体受体亲和力和药代动力学来确定的。同时,ADC中使用的连接子可以是可裂解的或不可裂解的。ADC疗法除了有效载荷的直接细胞毒性作用外,还包括抗体依赖性机制。这些机制包括抗体依赖性细胞毒性、补体依赖性细胞毒性和抗体依赖性细胞吞噬作用,以及“旁观者效应”,即一部分细胞毒性分子从靶细胞中扩散出来,对相邻细胞发挥细胞毒性作用。ADC的靶抗原预计在面向细胞外基质的癌细胞膜上表达,尽管新方法利用了与肿瘤相关细胞、肿瘤微环境或肿瘤脉管系统相关的抗原。ADC的这些靶抗原不仅决定了这些药物的疗效,还影响脱靶效应和相关不良反应。大多数与ADC相关的毒性都与脱靶效应有关。ADC耐药的潜在机制包括细胞内药物转运受阻、溶酶体加工功能失调以及细胞毒性分子通过ATP结合盒(ABC)转运蛋白流出。后一种机制在多药耐药肿瘤中尤为突出。ADC的一个重要局限性是偶联物进入肿瘤微环境以及将其递送至靶癌细胞的能力。癌组织的血管分布以及肿瘤周围血管周围形成的空间“结合位点屏障”是实体瘤ADC治疗的潜在挑战。随着研究工作集中在降低毒性、克服耐药性和改善药代动力学方面,预计癌症治疗的ADC选择将继续多样化,包括单一疗法和联合疗法。