Chen Yuwen, Lian Wenbin, Wu Lunzhe, Huang An'an, Zhang Deliang, Liu Bingchen, Qiu Yuangang, Wei Qucheng
Department of Cardiology, Second Affiliated Hospital, Zhejiang University School of Medicine, Hangzhou, 310009, China.
State Key Laboratory of Transvascular Implantation Devices, Hangzhou, 310009, China.
Cardiovasc Diabetol. 2025 Mar 29;24(1):147. doi: 10.1186/s12933-025-02692-x.
The Cardiovascular-Kidney-Metabolic (CKM) syndrome underscores the complex interactions among metabolic disorders, kidney disease, and cardiovascular conditions. Insulin resistance (IR) and inflammation are crucial in CKM syndrome development, but their combined effect in stages 0-3 remains unclear.
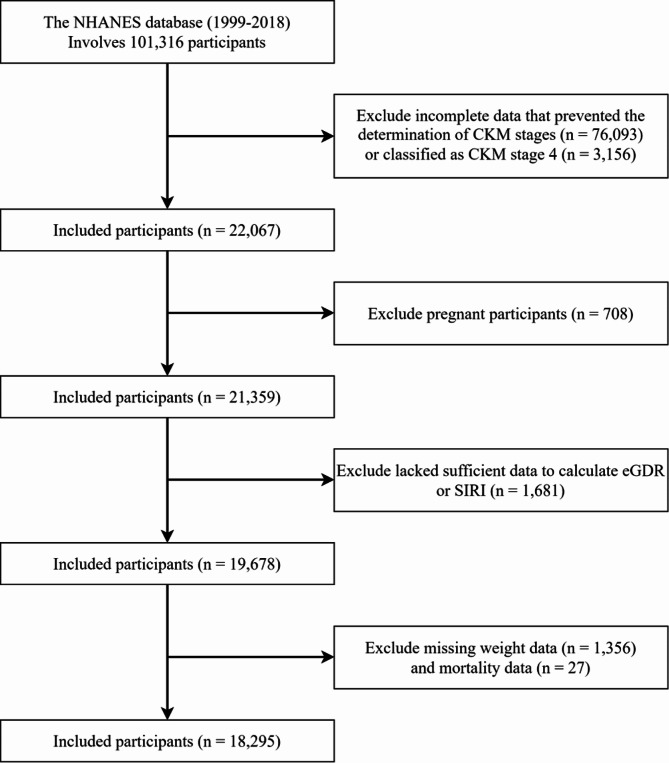
Using data from the National Health and Nutrition Examination Survey (NHANES), we included 18,295 participants with CKM syndrome stages 0-3 from 10 cycles between 1999 and 2018. IR was assessed using the estimated glucose disposal rate (eGDR), and systemic inflammation was evaluated using the Systemic Inflammation Response Index (SIRI). The primary endpoint was all-cause mortality, and the secondary endpoint was cardiovascular disease (CVD) mortality.
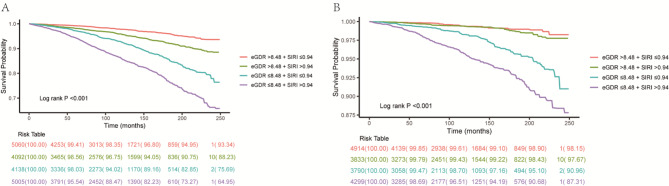
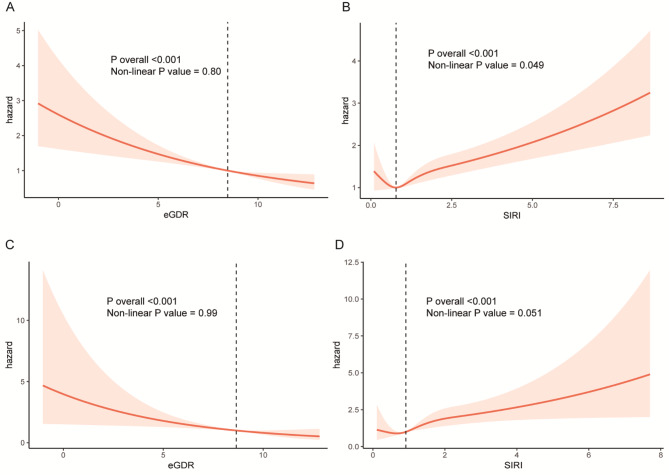
Over an average follow-up period of 121 months, we recorded 1,998 all-cause deaths and 539 CVD deaths. Both eGDR and SIRI were independent risk factors for mortality. The hazard ratios (HR) for eGDR were 0.90 (0.86, 0.94) for all-cause mortality and 0.85 (0.78, 0.93) for CVD mortality, per unit increase in eGDR. For SIRI, the HRs were 1.16 (1.11, 1.21) for all-cause mortality and 1.33 (1.19, 1.46) for CVD mortality, per unit increase in SIRI. Compared to individuals with high eGDR and low SIRI levels, those with low eGDR and high SIRI levels exhibited significantly higher mortality risks, with HRs of 1.97 (1.58, 2.44) for all-cause mortality and 2.35 (1.48, 3.73) for CVD mortality. Subgroup analysis revealed that the combined impact of eGDR and SIRI was particularly significant in patients under 60 years old.
In CKM syndrome stages 0-3, eGDR and SIRI have joint effect on mortality. Combining these markers can help identify high-risk individuals early, enabling timely monitoring and intervention to improve outcomes.
心血管 - 肾脏 - 代谢(CKM)综合征突显了代谢紊乱、肾脏疾病和心血管疾病之间复杂的相互作用。胰岛素抵抗(IR)和炎症在CKM综合征的发展中至关重要,但它们在0 - 3期的联合作用尚不清楚。
利用美国国家健康与营养检查调查(NHANES)的数据,我们纳入了1999年至2018年期间10个周期的18295名0 - 3期CKM综合征参与者。使用估计的葡萄糖处置率(eGDR)评估IR,使用全身炎症反应指数(SIRI)评估全身炎症。主要终点是全因死亡率,次要终点是心血管疾病(CVD)死亡率。
在平均121个月的随访期内,我们记录了1998例全因死亡和539例CVD死亡。eGDR和SIRI都是死亡率的独立危险因素。eGDR每增加一个单位,全因死亡率的风险比(HR)为0.90(0.86,0.94),CVD死亡率的HR为0.85(0.78,0.93)。对于SIRI,SIRI每增加一个单位,全因死亡率的HR为1.16(1.11,1.21),CVD死亡率的HR为1.33(1.19,1.46)。与eGDR高且SIRI水平低的个体相比,eGDR低且SIRI水平高的个体表现出显著更高的死亡风险,全因死亡率的HR为1.97(1.58,2.44),CVD死亡率的HR为2.35(1.48,3.73)。亚组分析显示,eGDR和SIRI的联合影响在60岁以下患者中尤为显著。
在CKM综合征0 - 3期,eGDR和SIRI对死亡率有联合作用。结合这些标志物有助于早期识别高危个体,以便及时进行监测和干预以改善预后。