Lee Jacqui A, Wise Jessika, Raudsepp Sara D, Paton Louise N, Powell Jan, Jina Kieran, Aldous Sally, Troughton Richard W, Adamson Philip D, Richards A Mark, Peacock W Frank, Januzzi James L, Erceg Noah, Koechlin Luca, Boeddinghaus Jasper, Lopez-Ayala Pedro, Mueller Christian, Than Martin P, Pickering John W, Pemberton Chris J
Department of Medicine, Christchurch Heart Institute, University of Otago, Christchurch, Riccarton Avenue, PO Box 4345, Christchurch 8011, New Zealand.
Upstream Medical Technologies, 3 Saint Aubyn Street, Devenport, Auckland 0624, New Zealand.
Eur Heart J Open. 2025 Mar 20;5(2):oeaf028. doi: 10.1093/ehjopen/oeaf028. eCollection 2025 Mar.
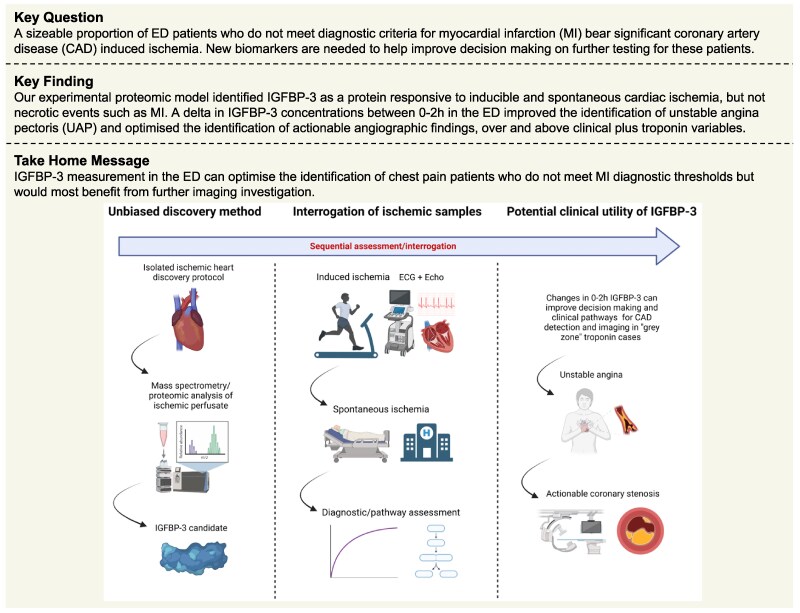
Among individuals presenting to the emergency department (ED) with chest pain, clinical uncertainty surrounds the appropriate identification of non-myocardial infarction (MI) individuals who would most benefit from objective functional/anatomical testing (e.g. imaging). We applied a proteomic biomarker discovery approach to identify novel candidates reflecting coronary artery disease (CAD) induced ischaemia that could translate to measurement in clinical samples.
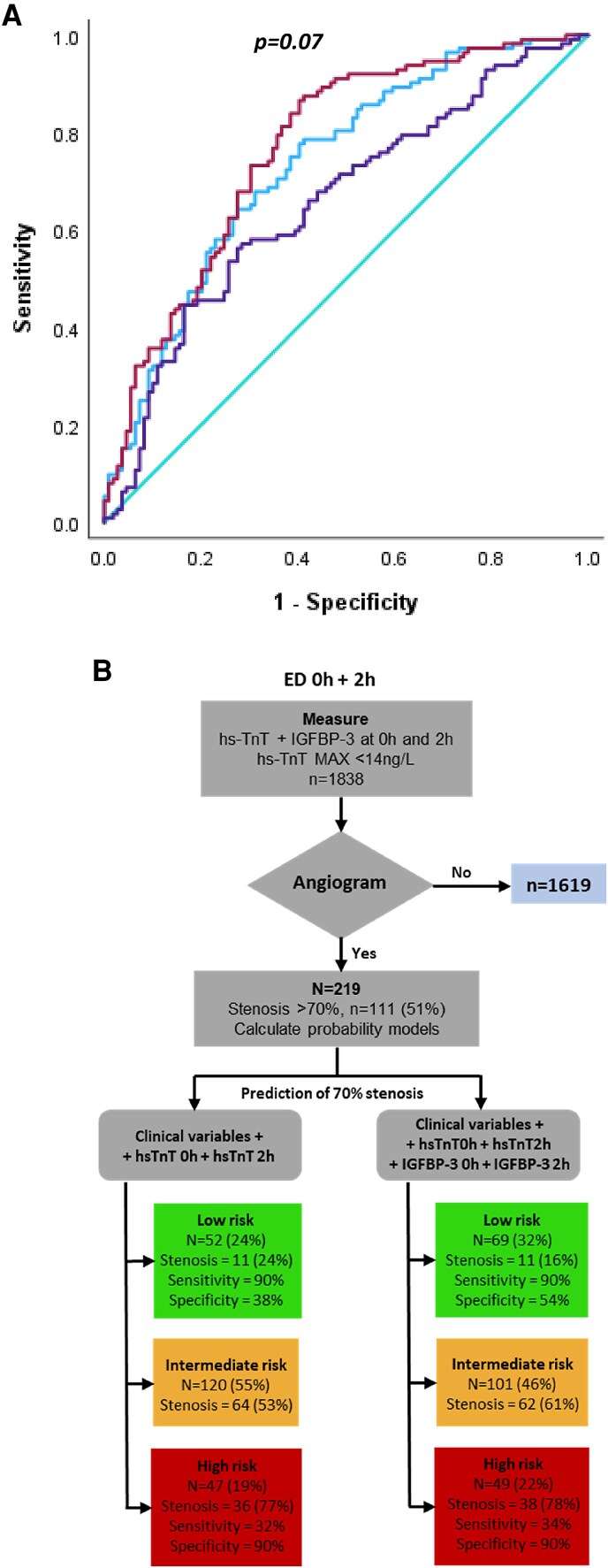
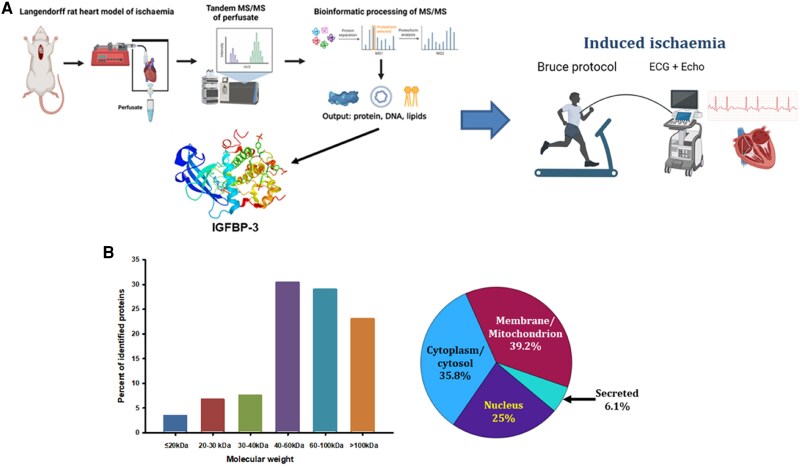
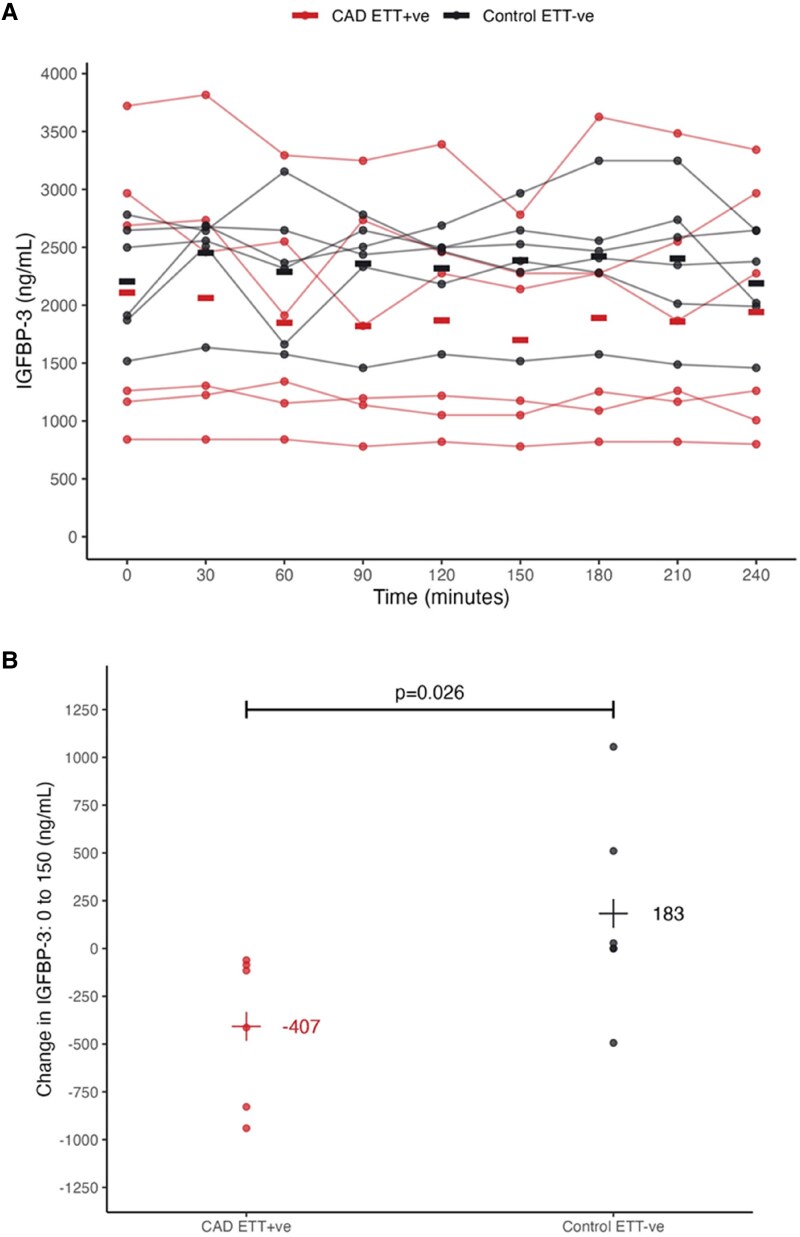
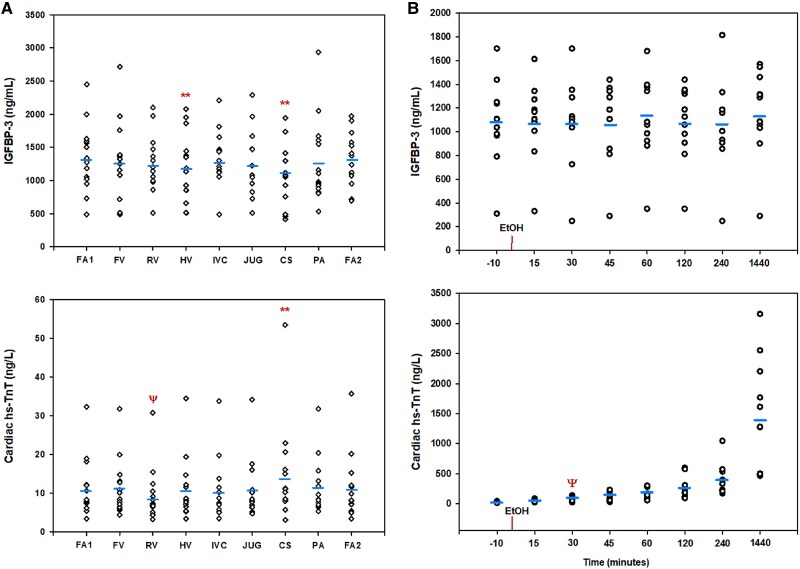
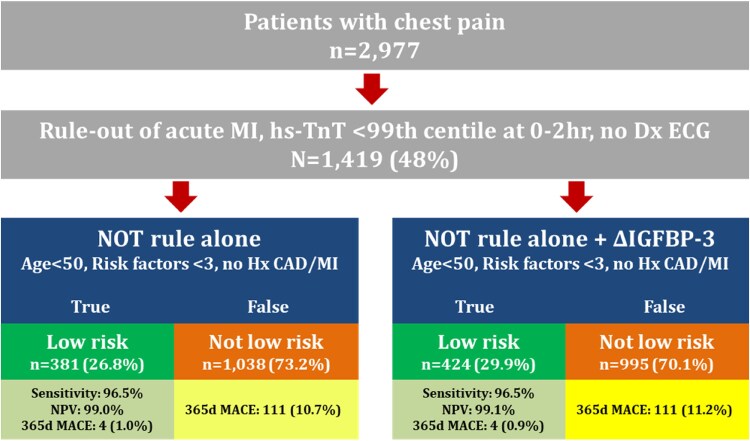
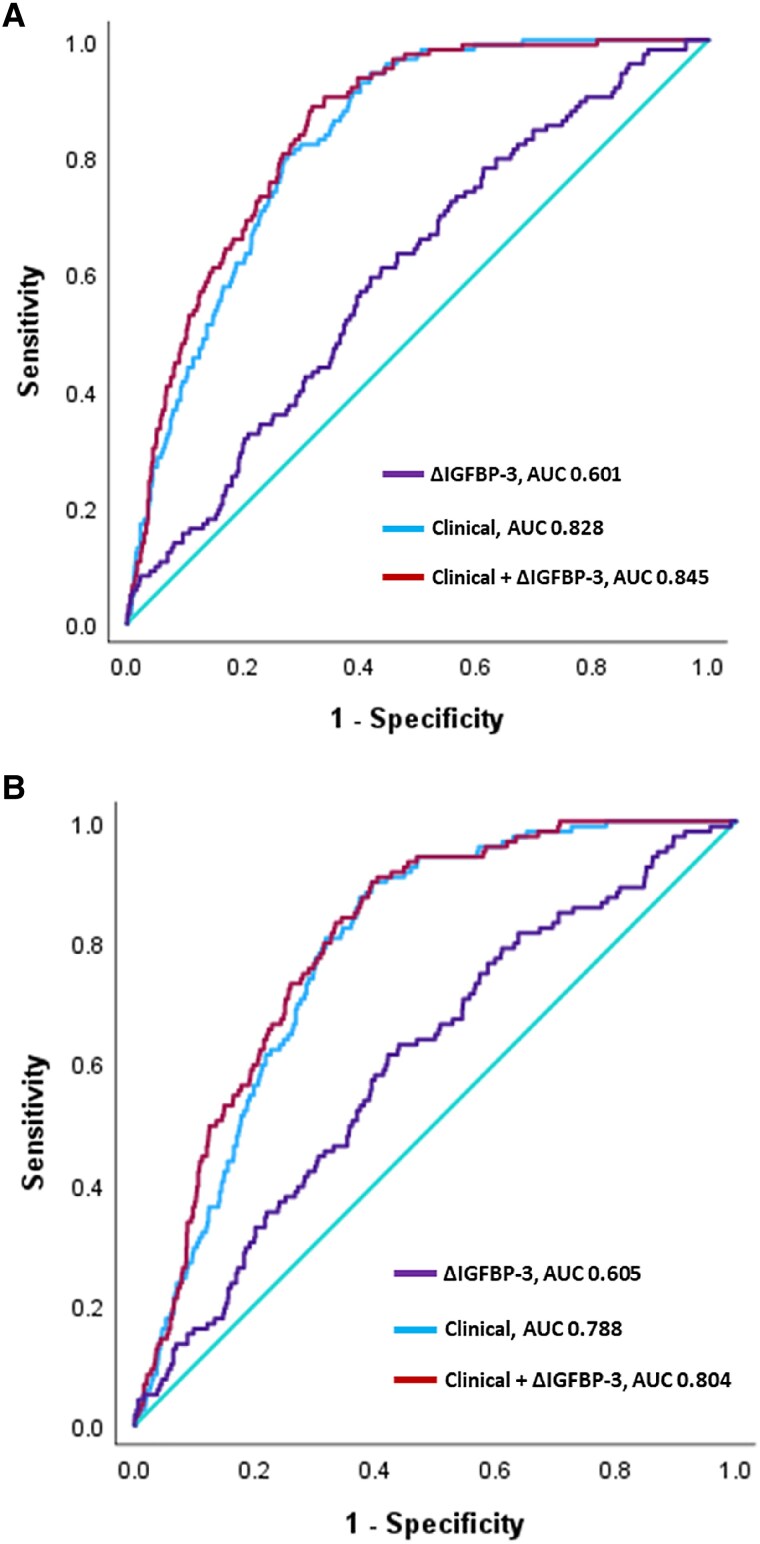
Mass spectroscopy (MS) of perfusate from an isolated rat heart model of cardiac ischaemia identified >100 novel protein biomarkers. A prominent candidate, insulin-like growth factor binding protein (IGFBP-3), was then interrogated for its ability to identify CAD-related ischaemia (e.g. positive cardiac stress test; unstable angina pectoris, UAP; arterial stenosis >70% on angiography) in multiple patient sample sets [cardiac stress testing, = 12; septal alcohol ablation (SAA), = 12; ED chest pain, = 2977]. In cardiac stress testing, a significant delta IGFBP-3 (ΔIGFBP-3) between 0 and 150 min was seen in positive, but not negative, tests ( = 0.03). In SAA, peripheral IGFBP-3 levels did not change over 24 h ( = 0.57). In ED patients, ΔIGFBP-3 between 0 and 2 h (i) identified more 365-day low-risk major adverse cardiac event cases (27-30%), (ii) provided 7% improvement in positive predictive value over a clinical model for the identification of unstable angina ( = 0.01), and (iii) was a significant, independent predictor of >70% stenosis on angiography, improving indeterminate risk prediction by 9% (95% CI 3-15%).
Our discovery approach has translated IGFBP-3 as a potential biomarker to identify significant CAD/ischaemia in patients who do not meet diagnostic thresholds for MI.
在因胸痛就诊于急诊科(ED)的患者中,对于如何恰当识别那些最能从客观功能/解剖学检查(如影像学检查)中获益的非心肌梗死(MI)患者,临床仍存在不确定性。我们采用蛋白质组学生物标志物发现方法,以识别反映冠状动脉疾病(CAD)所致缺血的新型候选标志物,这些标志物可转化用于临床样本检测。
对离体大鼠心脏缺血模型的灌注液进行质谱分析(MS),识别出100多种新型蛋白质生物标志物。随后,对一个突出的候选物胰岛素样生长因子结合蛋白(IGFBP - 3)在多个患者样本组中识别CAD相关缺血(如心脏负荷试验阳性;不稳定型心绞痛,UAP;血管造影显示动脉狭窄>70%)的能力进行了研究[心脏负荷试验,n = 12;间隔乙醇消融术(SAA),n = 12;ED胸痛患者,n = 2977]。在心脏负荷试验中,阳性试验(而非阴性试验)在0至150分钟之间出现了显著的IGFBP - 3变化量(ΔIGFBP - 3)(P = 0.03)。在SAA中,外周IGFBP - 3水平在24小时内未发生变化(P = 0.57)。在ED患者中,0至2小时之间的ΔIGFBP - 3:(i)识别出更多365天低风险主要不良心脏事件病例(27 - 30%),(ii)在识别不稳定型心绞痛的临床模型基础上,阳性预测值提高了7%(P = 0.01),并且(iii)是血管造影显示狭窄>70%的显著独立预测因子,将不确定风险预测提高了9%(95%CI 3 - 15%)。
我们的发现方法已将IGFBP - 3转化为一种潜在生物标志物,用于识别未达到MI诊断阈值的患者中的显著CAD/缺血情况。