Tumukunde Victor S, Sekitoleko Isaac, Opondo Charles, Nyirenda Moffat, Tann Cally J, Lawn Joy E, Medvedev Melissa M
Non-Communicable Disease Programme, Medical Research Council, Virus Research Institute and LSHTM Uganda Research Unit, PO Box 49, Entebbe, Uganda.
Department of Infectious Disease Epidemiology and International Health, London School of Hygiene & Tropical Medicine, Keppel Street, WC1E 7HT, London, UK.
BMC Pediatr. 2025 Apr 9;25(1):283. doi: 10.1186/s12887-025-05629-1.
Studies evaluating the impact of kangaroo mother care (KMC) on neonatal mortality and morbidity often rely on healthcare worker records or caregiver reports to measure intervention duration. However, the accuracy of these methods remains uncertain. We examined the validity of different methods of KMC duration measurement amongst neonates ≤ 2000 g in Uganda.
This observational study was embedded within the OMWaNA trial, which examined the impact of KMC on neonatal mortality before clinical stability. An independent observer (considered the gold standard) monitored neonates every 2 h to confirm KMC position, using an Android tablet-based application adapted from the EN-BIRTH study. The gold standard was compared to routine healthcare workers' charting and caregiver diary reports of KMC.
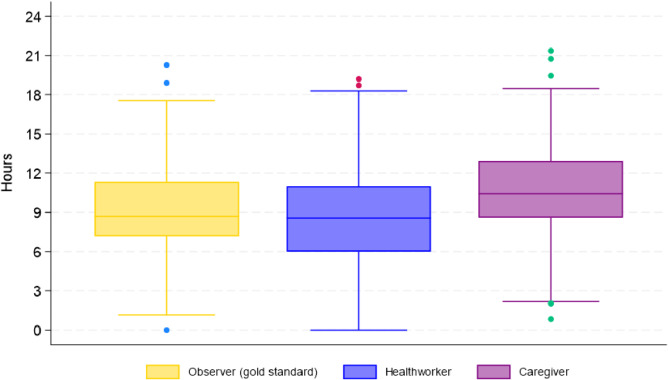
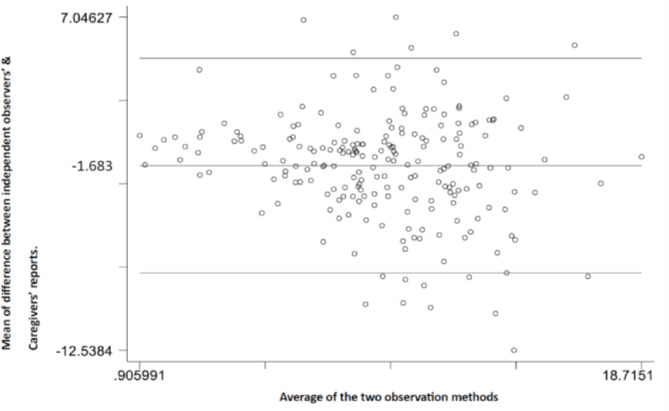
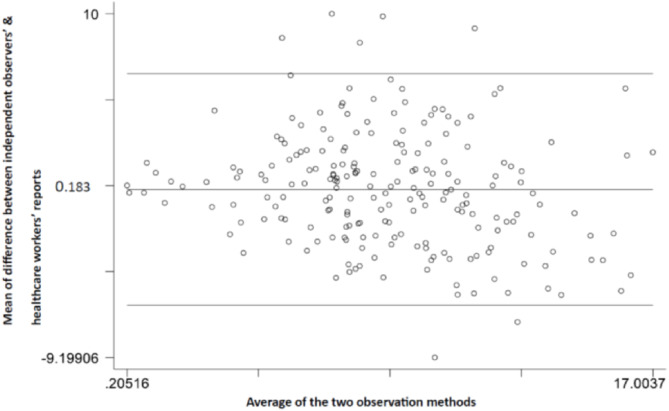
Among 222 caregiver-newborn pairs, 219 initiated KMC. The mean daily KMC duration recorded by the gold standard was 8·4 h (SD 3·5). Healthcare workers reported an average of 8·5 h (SD 4·0), while caregivers reported 10·4 h (SD 3·8). The mean difference was 0·2 h less for healthcare workers (95% CI -0·3 to 0·6) and 1·7 h more for caregivers (-2·1 to -1·3) compared to the gold standard. Agreement rates for individual KMC episodes were 55·2% (95% CI 54·4-55·9) for healthcare workers and 58·2% (57·2-59·0) for caregivers. Participants with a helper (substitute KMC provider) had longer daily duration compared to those without (mean difference 1·89 h [0·89 - 2·84]; p < 0·001).
Healthcare worker records provide a reasonably accurate estimate of KMC duration at the population level, supporting the integration of KMC indicators into national health information systems to facilitate monitoring and evaluation. The presence of a helper increases KMC duration, underscoring the need for research to identify strategies to increase family involvement.
评估袋鼠式护理(KMC)对新生儿死亡率和发病率影响的研究通常依赖医护人员记录或照料者报告来衡量干预时长。然而,这些方法的准确性仍不确定。我们在乌干达对体重≤2000克的新生儿中不同KMC时长测量方法的有效性进行了研究。
这项观察性研究纳入了OMWaNA试验,该试验研究了KMC在临床稳定前对新生儿死亡率的影响。一名独立观察者(视为金标准)每2小时监测一次新生儿,以确认KMC的实施情况,使用的是基于安卓平板电脑的应用程序,该程序改编自EN-BIRTH研究。将金标准与医护人员的常规记录以及照料者关于KMC的日记报告进行比较。
在222对照料者与新生儿组合中,219对开始了KMC。金标准记录的每日KMC平均时长为8.4小时(标准差3.5)。医护人员报告的平均时长为8.5小时(标准差4.0),而照料者报告的为10.4小时(标准差3.8)。与金标准相比,医护人员报告的平均差异少0.2小时(95%置信区间 -0.3至0.6),照料者报告的平均差异多1.7小时(-2.1至-1.3)。医护人员对单个KMC时段的一致率为55.2%(95%置信区间54.4 - 55.9),照料者为58.2%(57.2 - 59.0)。有帮手(替代KMC提供者)的参与者每日时长比没有帮手的参与者更长(平均差异1.89小时[0.89 - 2.84];p < 0.001)。
医护人员记录在人群层面提供了对KMC时长的合理准确估计,支持将KMC指标纳入国家卫生信息系统以促进监测和评估。帮手的存在会增加KMC时长,凸显了开展研究以确定增加家庭参与策略的必要性。