Ghoshal Uday C, Mustafa Uzma, Goenka Mahesh K, Kothalkar Srikant, Panday Vipin, Panday Ankita
Department of Gastroenterology, Sanjay Gandhi Postgraduate Institute of Medical Sciences, Lucknow, India.
Institute of Gastrosciences and Liver Transplantation, Apollo Multi-speciality Hospitals, Kolkata, India.
J Neurogastroenterol Motil. 2025 Apr 30;31(2):227-240. doi: 10.5056/jnm24049.
BACKGROUND/AIMS: Gastric dysrhythmias, loss of normal 3 cycles per minute (CPM) gastric myoelectrical activity (GMA), and variable loss of interstitial cells of Cajal are reported both in gastroparesis (GP) and functional dyspepsia (FD). We hypothesize that the patients with GP, and FD with normal gastric emptying (NGE) and delayed gastric emptying (DGE) may vary in symptom severity, and GMA profiles.
Symptoms and their severity were evaluated by gastroparesis cardinal symptom index (GCSI), Abell scoring, short-form Nepean dyspepsia index (SF-NDI), the World Health Organization quality of life, and Rome IV subtyping for FD. Solid-meal gastric emptying was assessed by nuclear scintigraphy. Water load satiety test (WLST)-based electrogastrography determined GMA.
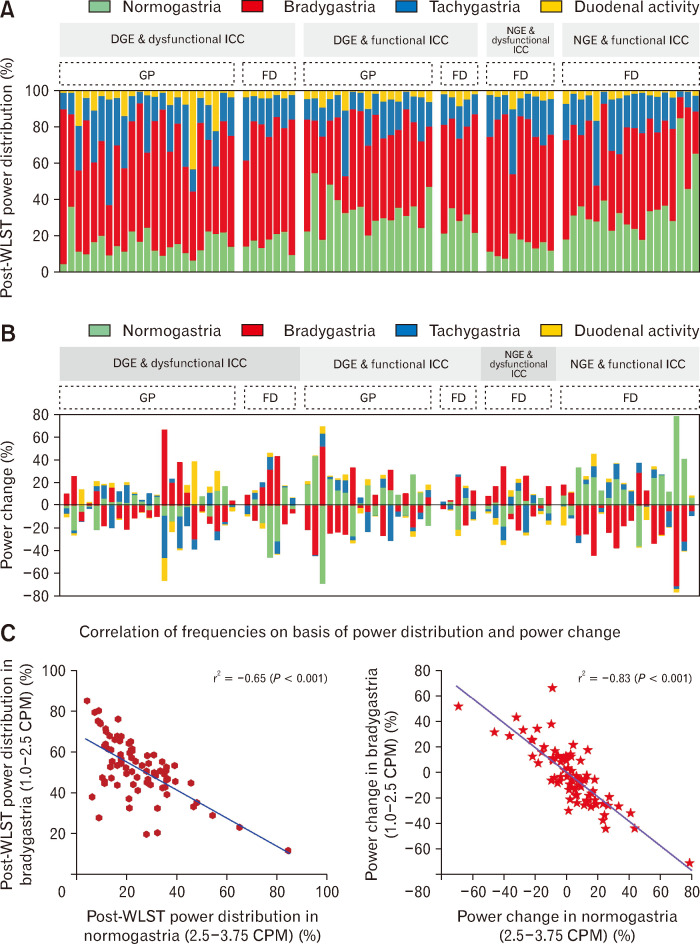
Patients with GP (n = 40) had higher GCSI than those with FD (n = 39; [12 DGE, 27 NGE] (2.79 [2.17-3.33] vs 1.67 [0.83-2.61] vs 0.83 [0.55-1.93]; < 0.001, in GP vs FD-NGE vs FD-DGE, respectively), severe Abell grade (Grade III in 17 [43%] vs 0% vs 0%, in GP vs FD-NGE vs FD-DGE, respectively), severe SF-NDI (80.5 [63.5-102.5] vs 50 [27-91] vs 30 [21.25-45.5]); and poor QOL. Sixteen (40%) GP had impaired gastric accommodation (< 238 mL). Post-WLST 3 CPM normal/hypernormal GMA was observed in 17 (42%), 18 (67%), and 5 (42%) patients with GP, FD (NGE), and FD (DGE), respectively; and 3 CPM hyponormal in remaining patients in each group. Post-WLST dysrhythmia was comparable.
WLST-electrogastrography coupled with GE study may distinguish between normal/dysrhythmic GMA revealing pathophysiologicalphenotypes of GP and FD. Analysing extent of power change in normogastric, and dysrhythmic frequencies may comprehensively elucidate disease severity.
背景/目的:胃轻瘫(GP)和功能性消化不良(FD)患者均有胃节律紊乱、正常每分钟3个周期(CPM)的胃肌电活动(GMA)丧失以及 Cajal 间质细胞不同程度的丧失。我们假设,GP患者以及胃排空正常(NGE)和胃排空延迟(DGE)的FD患者在症状严重程度和GMA特征方面可能存在差异。
通过胃轻瘫主要症状指数(GCSI)、阿贝尔评分、简化版内皮恩消化不良指数(SF-NDI)、世界卫生组织生活质量评估以及FD 的罗马IV亚型分类来评估症状及其严重程度。通过核素闪烁扫描评估固体餐胃排空情况。基于水负荷饱腹感试验(WLST)的胃电图测定GMA。
GP患者(n = 40)的GCSI高于FD患者(n = 39;[12例DGE,27例NGE](分别为2.79 [2.17 - 3.33] 对比1.67 [0.83 - 2.61] 对比0.83 [0.55 - 1.93];P < 0.001,分别为GP对比FD - NGE对比FD - DGE)),阿贝尔分级严重(分别为17例[43%]为III级对比FD - NGE组0%对比FD - DGE组0%),SF-NDI严重(80.5 [63.5 - 102.5] 对比50 [