Pu Wenji, Li Shasha, Zhang Jinliang, Huang Jijie, Li Jishi, Jiang Yong, Xu Zhiyuan, Yi Fan, Lan Yuling, Xiao Qin, Chen Wenqi, Jin Jing
Department of Clinical Oncology, The University of Hong Kong-Shenzhen Hospital, Shenzhen, China.
National Cancer Center/National Clinical Research Center for Cancer/Cancer Hospital & Shenzhen Hospital, Chinese Academy of Medical Sciences and Peking Union Medical College, Shenzhen, China.
Front Immunol. 2025 Mar 26;16:1566939. doi: 10.3389/fimmu.2025.1566939. eCollection 2025.
Immune checkpoint inhibitors (ICIs) plus fluorouracil-based chemotherapy (Chemo) have been approved as an initial treatment strategy for metastatic or recurrent human epidermal growth factor receptor 2 (HER2)-negative gastric cancer (GC) or gastroesophageal junction cancer (GEJC). However, since programmed cell death protein-1 (PD-1) or its ligand 1 (PD-L1) inhibitors have just recently been investigated for the treatment of unresectable GC/GEJC, there is ongoing debate regarding their safety and effectiveness for prespecified subgroups. The purpose of this research is to establish a foundation toward stratified decision-making by methodically assessing the merits and drawbacks of PD-1/PD-L1 inhibitors combined with chemo in the clinical utilization of advanced HER2-negative GC/GEJC according to certain prominent large-scale randomized controlled trials (RCTs). In addition, we limitedly explored the favorable short-term efficacy of PD-1/CTLA-4 bispecific antibodies for the above-mentioned tumors.
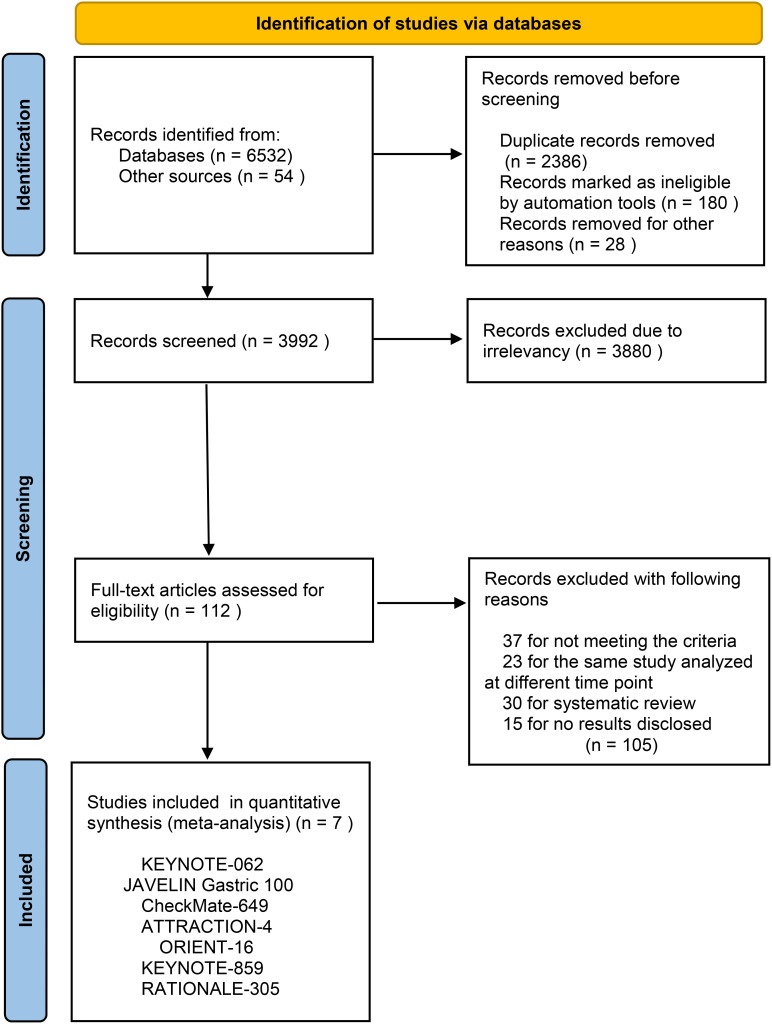
The researchers retrieved several databases, including PubMed, Embase, Web of Science, ClinicalTrials.gov, and the Cochrane Library, to collect all the relevant literature published since the establishment of the databases until October 30, 2024, and then screened to determine the qualified literature and extracted the relevant information. We only included RCTs for PD-1/PD-L1 inhibitors with or without chemo in advanced GC or GEJC. The primary endpoints were overall survival (OS), progression-free survival (PFS), and objective response rate (ORR). A subgroup analysis for the median overall survival (mOS) was conducted for the following variables: microsatellite instability (MSI) status, PD-L1 expression, combined positive scores (CPS), metastasis status, and primary tumor location. When moderate heterogeneity was found, a random-effect model was applied. The outcome indicators were then statistically analyzed, taking advantage of Review Manager 5.4. Hazard ratio (HR) and risk ratio (RR) were selected as the effect values for statistical analysis.
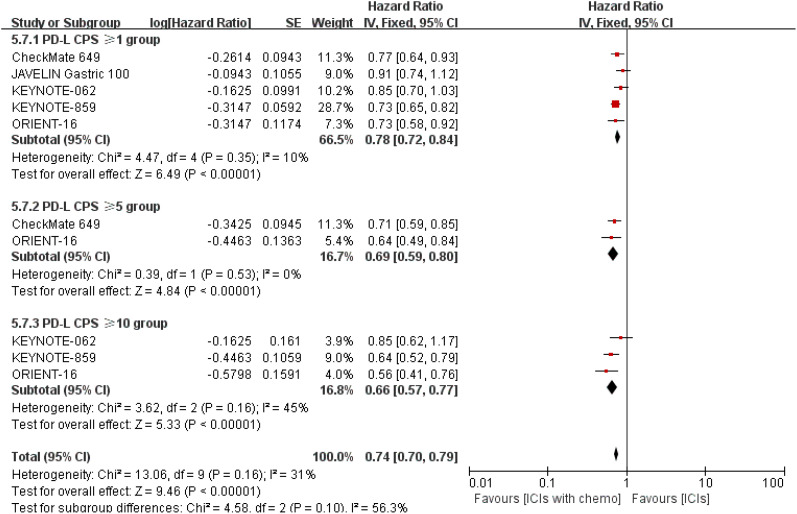
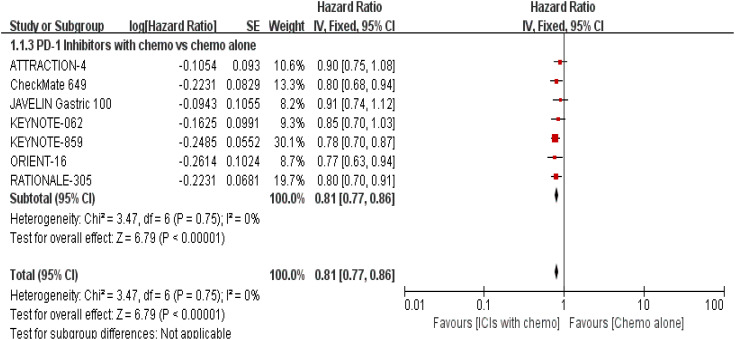
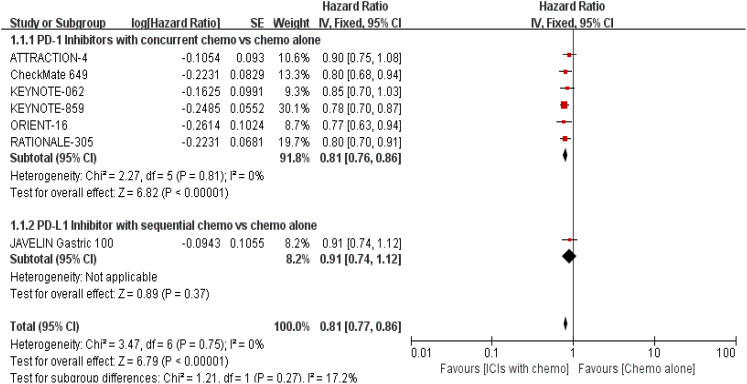
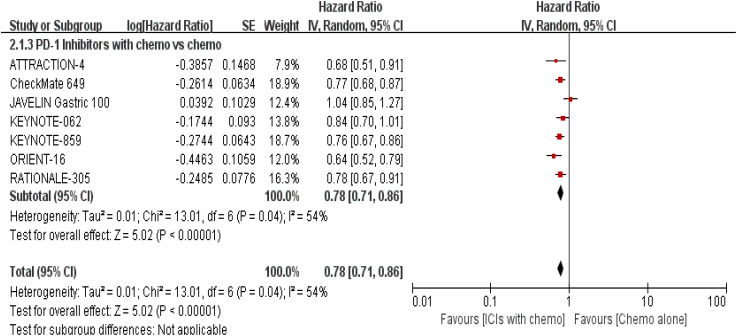
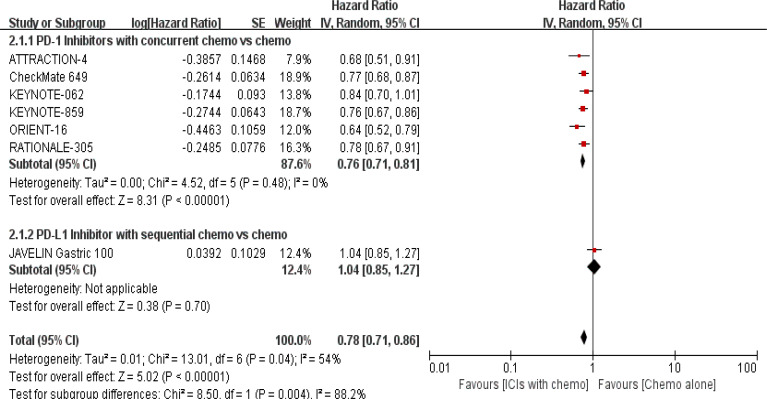
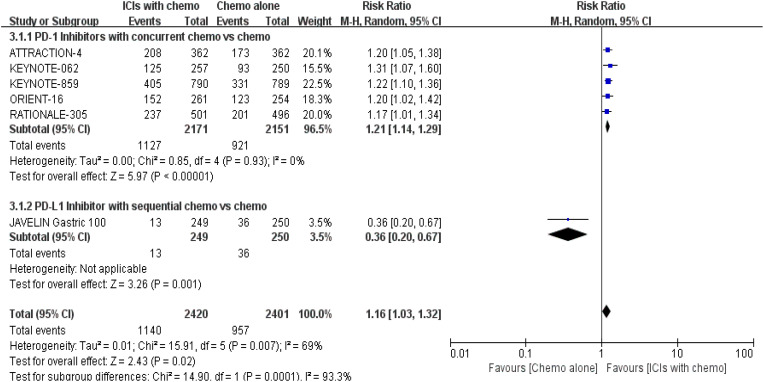
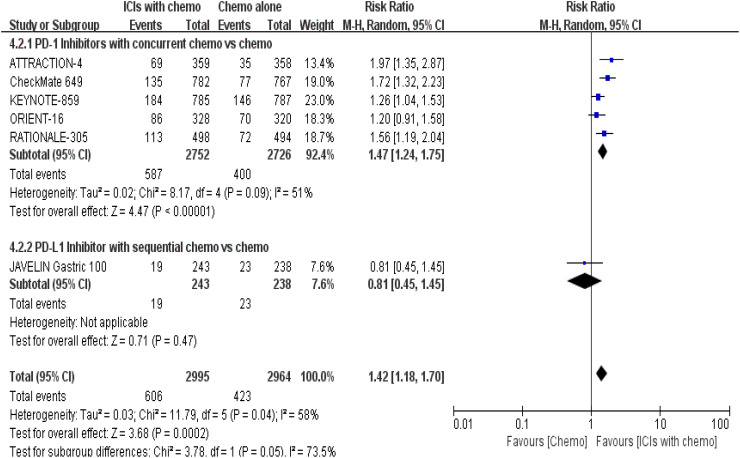
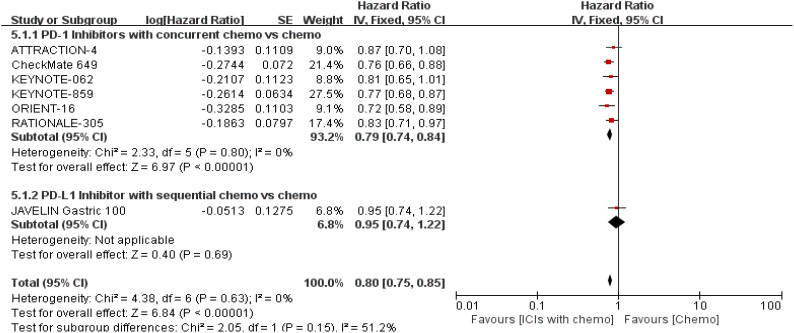
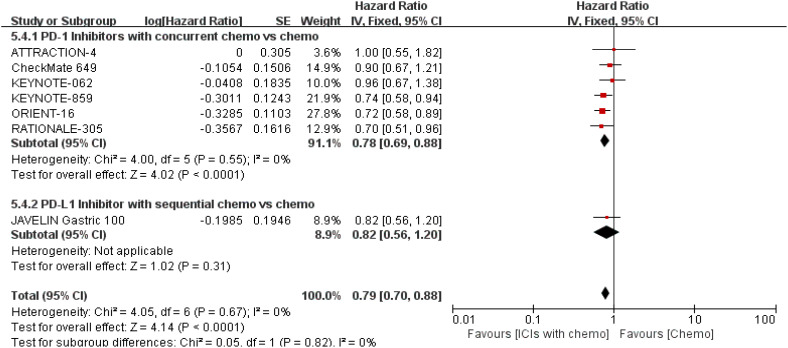
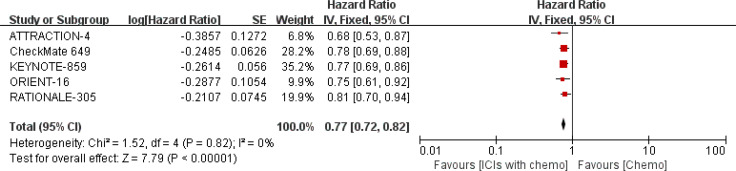
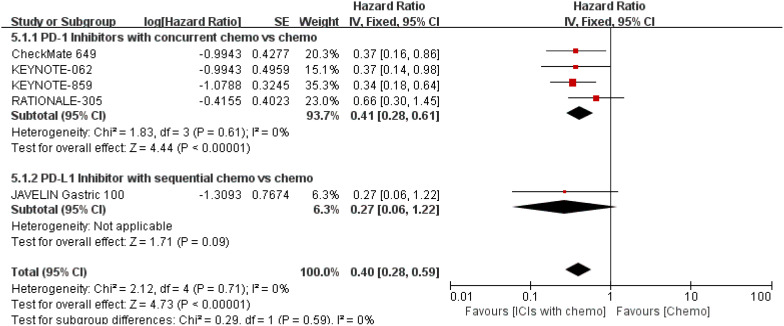
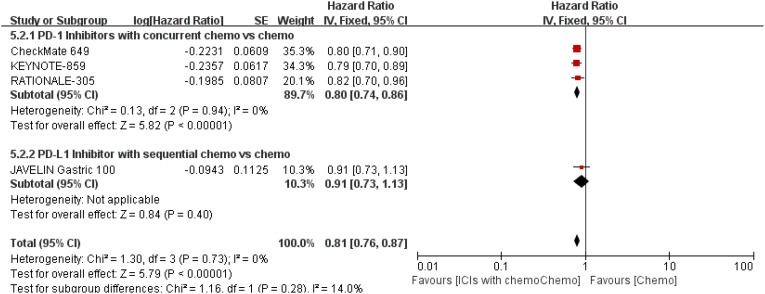
A total of 7 eligible RCTs and 6537 participants were included in this meta-analysis. Combining PD-1/PD-L1 inhibitors with chemo significantly improved patients' OS compared with chemo alone, especially in the tumor cell PD-L1 expression ≥ 1% [HR = 0.62, 95% CI (0.48, 0.81); a p-value = 0.0004], PD-L1 CPS ≥ 10 [HR = 0.66, 95% CI (0.57, 0.77); a p-value < 0.00001], and MSI-H subgroups [HR = 0.40, 95% CI (0.28, 0.59); a p-value < 0.00001]. Moreover, distinct primary tumor location (GC or GEJC) and the presence of liver metastases could also benefit from the additive or sustained effect of anti-cancer chemo-immunotherapy.
For patients with advanced HER2-negative GC/GEJC, PD-1/PD-L1 inhibitors in combination with chemo have almost demonstrated consistent synergistic anti-tumor benefits to survival outcomes when compared to chemo alone. However, the subgroup analysis in this meta-study revealed that neither PD-L1 expression level nor MSI status could fully predict the efficacy of the dual treatment model but faced a higher possibility of serious treatment-related adverse events (sTRAEs), particularly in the synchronous therapy arm. Therefore, urging the need for more investigations into the development of collaborative prognostic forecasting models for achieving precise stratification, established harmonized testing standards and methods for PD-L1 expression and positivity, optimal CPS threshold for benefits, as well as alternative molecular biomarkers for the reason that certain indicators alone may not discriminate responders clearly. Lastly, dual anti-therapy might be a useful tactic for the population with low PD-L1 expression in the future.
免疫检查点抑制剂(ICIs)联合氟尿嘧啶类化疗(化疗)已被批准作为转移性或复发性人表皮生长因子受体2(HER2)阴性胃癌(GC)或胃食管交界癌(GEJC)的初始治疗策略。然而,由于程序性细胞死亡蛋白1(PD-1)或其配体1(PD-L1)抑制剂最近才被研究用于治疗不可切除的GC/GEJC,关于其对特定亚组的安全性和有效性仍存在争议。本研究的目的是通过系统评估PD-1/PD-L1抑制剂联合化疗在晚期HER2阴性GC/GEJC临床应用中的优缺点,为分层决策奠定基础,参考某些著名的大规模随机对照试验(RCT)。此外,我们还有限地探索了PD-1/CTLA-4双特异性抗体对上述肿瘤的良好短期疗效。
研究人员检索了多个数据库,包括PubMed、Embase、Web of Science、ClinicalTrials.gov和Cochrane图书馆,以收集自数据库建立至2024年10月30日发表的所有相关文献,然后进行筛选以确定合格文献并提取相关信息。我们仅纳入了晚期GC或GEJC中使用或未使用化疗的PD-1/PD-L1抑制剂的RCT。主要终点为总生存期(OS)、无进展生存期(PFS)和客观缓解率(ORR)。对以下变量进行了中位总生存期(mOS)的亚组分析:微卫星不稳定性(MSI)状态、PD-L1表达、联合阳性评分(CPS)、转移状态和原发肿瘤位置。当发现中度异质性时,应用随机效应模型。然后利用Review Manager 5.4对结果指标进行统计分析。选择风险比(HR)和风险率(RR)作为统计分析的效应值。
本荟萃分析共纳入7项合格的RCT和6537名参与者。与单纯化疗相比,PD-1/PD-L1抑制剂联合化疗显著改善了患者的OS,尤其是在肿瘤细胞PD-L1表达≥1%[HR = 0.62,95%CI(0.48,0.81);p值 = 0.0004]、PD-L1 CPS≥10[HR = 0.66,95%CI(0.57,0.77);p值 < 0.00001]和MSI-H亚组[HR = 0.40,95%CI(0.28,0.59);p值 < 0.00001]中。此外,不同的原发肿瘤位置(GC或GEJC)和肝转移的存在也可从抗癌化疗免疫治疗的附加或持续效应中获益。
对于晚期HER2阴性GC/GEJC患者,与单纯化疗相比,PD-1/PD-L1抑制剂联合化疗几乎已证明对生存结局具有一致的协同抗肿瘤益处。然而,本荟萃研究中的亚组分析显示,PD-L1表达水平和MSI状态均不能完全预测双重治疗模式的疗效,但面临更高的严重治疗相关不良事件(sTRAEs)可能性,尤其是在同步治疗组。因此,迫切需要更多研究来开发协作性预后预测模型以实现精确分层,建立统一的PD-L1表达和阳性检测标准及方法、获益的最佳CPS阈值,以及替代分子生物标志物,因为某些指标单独可能无法清晰区分反应者。最后,双重抗治疗可能是未来PD-L1低表达人群的一种有用策略。