Cai Yuzhu, Yang Mingwen, Liu Xinghui, Zhang Lingli, Wang Jun, Sun Yingying
Department of Anesthesiology, Anhui Provincial Children's Hospital, Hefei, 230051, China.
BMC Anesthesiol. 2025 Apr 10;25(1):172. doi: 10.1186/s12871-025-03053-7.
This study aimed to evaluate the effects of caudal block anesthesia with hydromorphone-ropivacaine compared to ropivacaine alone on postoperative immune function and pain management in children undergoing hypospadias surgery.
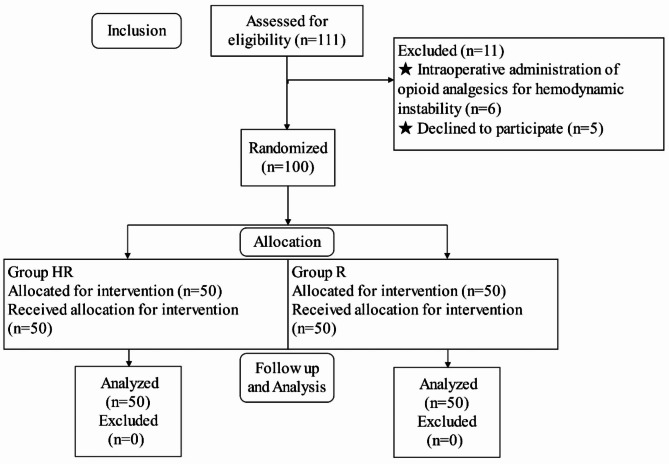
A total of 100 pediatric patients were randomly assigned to two groups: the Hydromorphone-Ropivacaine (HR) group and the Ropivacaine (R) group for caudal block anesthesia, with 50 patients in each group. The R group received 0.25% ropivacaine at a dose of 1 ml/kg, while the HR group received 0.25% ropivacaine (1 ml/kg) combined with hydromorphone (10 µg/kg). The maximum dose for both groups was capped at 30 ml (1 ml/kg). Anesthesia induction included intravenous administration of pentobarbital (0.01 mg/kg) and dexamethasone (0.15 mg/kg), followed by sevoflurane inhalation. All patients underwent ultrasound-guided caudal block anesthesia administered by the same anesthetist. Primary outcomes included the distribution of T lymphocyte subsets (CD3+, CD4+, CD8+, and CD4+/CD8 + ratios) measured at five time points: pre-anesthesia (T0), end of surgery (T1), 24 h postoperatively (T2), 48 h postoperatively (T3), and 72 h postoperatively (T4). Secondary outcomes included postoperative pain scores assessed using the Modified Children's Hospital of Eastern Ontario Pain Scale (M-CHEOPS) at 1, 6, 12, 18, and 24 h postoperatively, sedation levels evaluated using the Ramsay sedation scale at the same time points, and the incidence of postoperative adverse events.
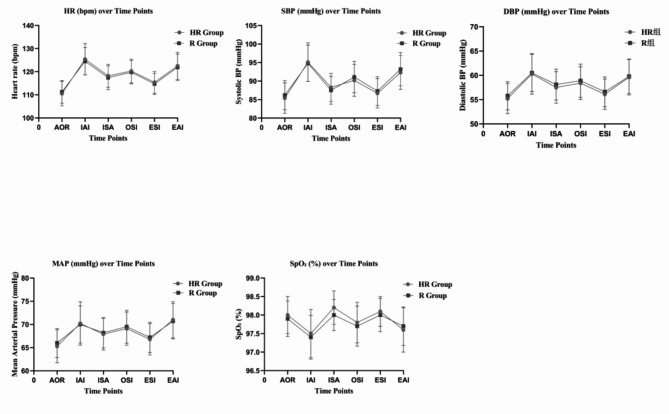
The HR group exhibited significant reductions in CD3, CD4, and CD4/CD8 ratios at T1, T2, and T3 compared to baseline (T0) (p < 0.001). At all postoperative time points (T1, T2, T3, T4), the HR group demonstrated significantly higher levels of CD3, CD4, and CD4/CD8 ratios compared to the R group (p < 0.001). By T4 (72 h postoperatively), immune markers in the HR group had largely normalized to baseline levels, whereas those in the R group remained significantly lower (p < 0.001). Postoperative pain, assessed using the Modified Children's Hospital of Eastern Ontario Pain Scale (M-CHEOPS), was significantly lower in the HR group at 6, 12, and 18 h postoperatively compared to the R group (p < 0.001). The HR group also exhibited a longer duration of analgesia and required fewer doses of rescue analgesia within the first 24 h postoperatively (p = 0.046). Sedation levels, evaluated using the Ramsay sedation scale, showed significant differences between the groups at 1 h (p = 0.0087) and 6 h (p < 0.0001) postoperatively, with higher sedation scores observed in the HR group. There were no significant differences in heart rate, systolic blood pressure, diastolic blood pressure, mean arterial pressure, or oxygen saturation between the groups at any time point (p > 0.05). No significant differences were observed between the two groups in terms of postoperative adverse reactions (all p > 0.05).
Caudal block anesthesia with hydromorphone-ropivacaine offers enhanced postoperative pain relief and a lesser impact on immune function compared to ropivacaine alone in children undergoing hypospadias surgery. Further studies are warranted to explore the long-term effects on immune function.
本研究旨在评估与单独使用罗哌卡因相比,氢吗啡酮 - 罗哌卡因骶管阻滞麻醉对小儿尿道下裂手术患者术后免疫功能和疼痛管理的影响。
总共100例儿科患者被随机分为两组:氢吗啡酮 - 罗哌卡因(HR)组和罗哌卡因(R)组进行骶管阻滞麻醉,每组50例患者。R组接受0.25%罗哌卡因,剂量为1 ml/kg,而HR组接受0.25%罗哌卡因(1 ml/kg)联合氢吗啡酮(10 μg/kg)。两组的最大剂量上限为30 ml(1 ml/kg)。麻醉诱导包括静脉注射戊巴比妥(0.01 mg/kg)和地塞米松(0.15 mg/kg),随后吸入七氟醚。所有患者均由同一名麻醉医生进行超声引导下的骶管阻滞麻醉。主要结局包括在五个时间点测量的T淋巴细胞亚群(CD3 +、CD4 +、CD8 +和CD4+/CD8 +比值)分布:麻醉前(T0)、手术结束时(T1)、术后24小时(T2)、术后48小时(T3)和术后72小时(T4)。次要结局包括术后1、6、12、18和24小时使用改良的安大略东部儿童医院疼痛量表(M-CHEOPS)评估的术后疼痛评分,同时使用Ramsay镇静量表评估的镇静水平,以及术后不良事件的发生率。
与基线(T0)相比,HR组在T1、T2和T3时CD3、CD4和CD4/CD8比值显著降低(p < 0.001)。在所有术后时间点(T1、T2、T3、T4),HR组的CD3、CD4和CD4/CD8比值水平均显著高于R组(p < 0.001)。到T4(术后72小时)时,HR组的免疫标志物已基本恢复到基线水平,而R组的免疫标志物仍显著较低(p < 0.001)。使用改良的安大略东部儿童医院疼痛量表(M-CHEOPS)评估,HR组术后6、12和18小时的术后疼痛明显低于R组(p < 0.001)。HR组的镇痛持续时间也更长,且术后24小时内所需的补救镇痛剂量更少(p = 0.046)。使用Ramsay镇静量表评估,两组在术后1小时(p = 0.0087)和6小时(p < 0.0001)的镇静水平存在显著差异,HR组的镇静评分更高。两组在任何时间点的心率、收缩压、舒张压、平均动脉压或血氧饱和度均无显著差异(p > 0.05)。两组在术后不良反应方面未观察到显著差异(所有p > 0.05)。
与单独使用罗哌卡因相比,氢吗啡酮 - 罗哌卡因骶管阻滞麻醉在小儿尿道下裂手术中可提供更好的术后疼痛缓解,且对免疫功能的影响较小。有必要进一步研究以探讨其对免疫功能的长期影响。