Besnard Aurélie, Pelle Juliette, Pruvost-Robieux Estelle, Ginguay Antonin, Vigneron Clara, Pène Frédéric, Mira Jean-Paul, Cariou Alain, Benghanem Sarah
Medical ICU, Cochin Hospital, Assistance Publique - Hôpitaux de Paris (AP‑HP) AP-HP Centre Université Paris Cité, 27 Rue du Faubourg Saint‑Jacques, 75014, Paris, France.
University Paris Cité - Medical School, Paris, France.
Crit Care. 2025 Apr 11;29(1):149. doi: 10.1186/s13054-025-05378-8.
Prognostic markers of good neurological outcome after cardiac arrest (CA) remain limited. We aimed to evaluate the prognostic value of neuron-specific enolase (NSE), electroencephalogram (EEG) and somatosensory evoked potentials (SSEP) in predicting good outcome, assessed separately and in combination.
A retrospective study was conducted in a tertiary CA center, using a prospective registry. We included all patients comatose after discontinuation of sedation and with one EEG and NSE blood measurement at 24, 48 or/and 72 h after CA. The primary outcome was favorable neurological outcome at three months, a Cerebral Performance Categories (CPC) scale 1-2 defining a good outcome.
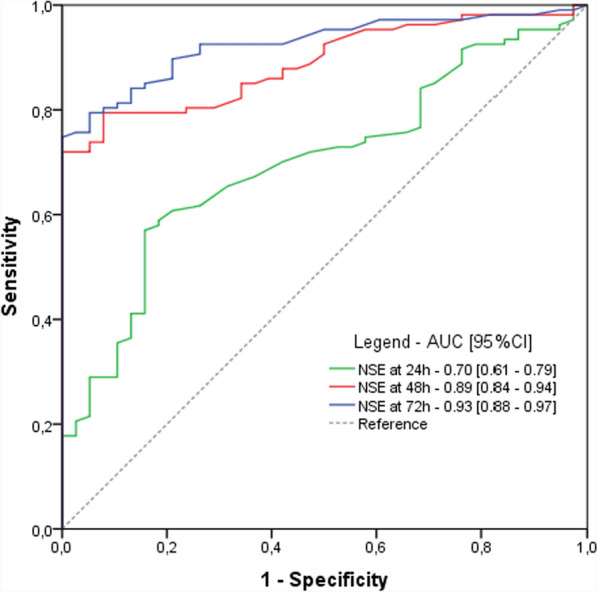
Between January 2017 and April 2024, 215 patients were included. Participants were 63 years old (IQR [52-73]), and 73% were male. At 3 months, 54 patients (25.1%) had a good outcome. Compared to the poor outcome group, NSE blood levels were significantly lower in the good outcome group at 24 h (39 IQR[27-45] vs 54 IQR[37-82]µg/L, p < 0.001), 48 h (26 [18-43] vs 107 [54-227]µg/L, p < 0.001) and 72 h (20 µg/L IQR [15-30] vs 184 µg/l IQR [60-300], p < 0,001). Normal NSE (i.e., < 17 µg/L) at 24 h was highly predictive of good outcome, with a predictive positive value (PPV) of 71% despite a sensitivity (Se) of 9%. The best cut-off values for NSE at 24, 48 and 72 h were below 45.5, 51.5 and 41.5 µg/L, yielding PPV of 64%, 80% and 83% and sensitivities of 74%, 93% and 90%, respectively. A decreasing trend in NSE levels between 24 and 72 h was also highly predictive of good outcome (PPV 82%, Se 81%). A benign EEG pattern was more frequently observed in the good outcome group (87.1 vs 14.9%, p < 0.001) and predicted a good outcome with a PPV of 72% and a Se of 94%. Regarding SSEPs, a bilateral N20-baseline amplitude > 0.85 µV was predictive of good outcome (PPV 75%, Se 100%). The combination of NSE < 51.5 µg/l at 48 h, a decreasing NSE trend between 24 and 72 h and a benign EEG showed the best predictive value (PPV 96%, Se 76%).
In comatose patients after CA, a low NSE levels at 24, 48 h or 72 h, a decreasing trend in NSE over time, a benign EEG and a high N20 amplitude are robust markers of favorable outcome, reducing prognosis uncertainty.
心脏骤停(CA)后良好神经功能预后的预测指标仍然有限。我们旨在评估神经元特异性烯醇化酶(NSE)、脑电图(EEG)和体感诱发电位(SSEP)在预测良好预后方面的价值,分别评估及联合评估。
在一家三级CA中心进行了一项回顾性研究,使用前瞻性登记册。我们纳入了所有在停用镇静剂后昏迷且在CA后24、48或/和72小时进行了一次EEG和NSE血液检测的患者。主要结局是三个月时良好的神经功能预后,脑功能类别(CPC)量表1-2定义为良好预后。
2017年1月至2024年4月期间,共纳入215例患者。参与者年龄为63岁(四分位间距[IQR][52-73]),73%为男性。在3个月时,54例患者(25.1%)预后良好。与预后不良组相比,良好预后组在24小时(39[IQR][27-45]对54[IQR][37-82]μg/L,p<0.001)、48小时(26[18-43]对107[54-227]μg/L,p<0.001)和72小时(20μg/L[IQR][15-30]对184μg/L[IQR][60-300],p<0.001)时的NSE血液水平显著较低。24小时时NSE正常(即<17μg/L)对良好预后具有高度预测性,尽管敏感性(Se)为9%,但预测阳性值(PPV)为71%。24、48和72小时时NSE的最佳截断值分别低于45.5、51.5和41.5μg/L,PPV分别为64%、80%和83%,敏感性分别为74%、93%和90%。24至72小时期间NSE水平呈下降趋势对良好预后也具有高度预测性(PPV 82%,Se 81%)。良好预后组更常观察到良性EEG模式(87.1%对14.9%,p<0.001),预测良好预后的PPV为72%,Se为94%。关于SSEP,双侧N20基线振幅>0.85μV对良好预后具有预测性(PPV 75%,Se 100%)。48小时时NSE<51.5μg/L、24至72小时期间NSE呈下降趋势以及良性EEG的组合显示出最佳预测价值(PPV 96%,Se 76%)。
在CA后的昏迷患者中,24、48或72小时时低NSE水平、NSE随时间下降趋势、良性EEG和高N20振幅是良好预后的可靠指标,可减少预后的不确定性。